

Surgical Approaches for Possible Positions of an Olfactory Implant to Stimulate the Olfactory Bulb
- PMID: 36996786
- PMCID: PMC10627492
- DOI: 10.1159/000529563
Surgical Approaches for Possible Positions of an Olfactory Implant to Stimulate the Olfactory Bulb
Abstract
Introduction: Current scientific developments seem to allow for an "olfactory implant" in analogy to cochlear implants. However, the position and surgical approaches for electrical stimulation of the olfactory system are unclear.
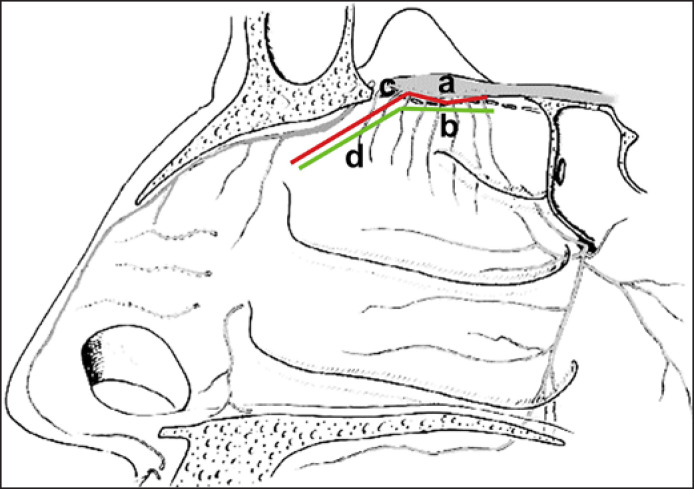
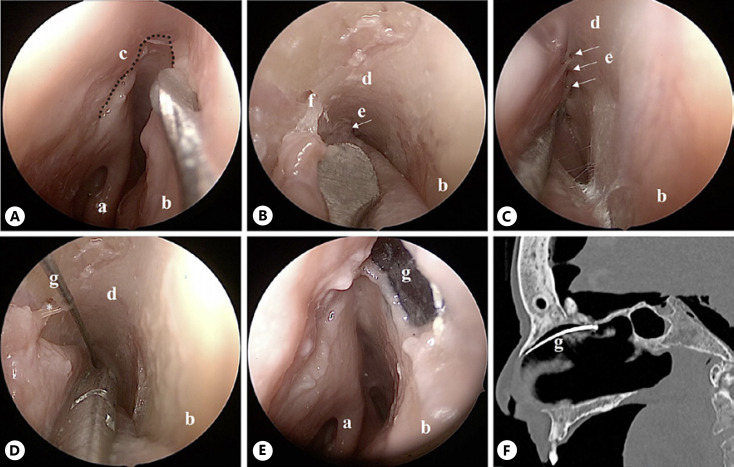
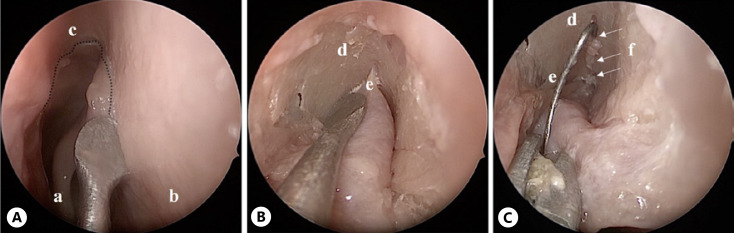
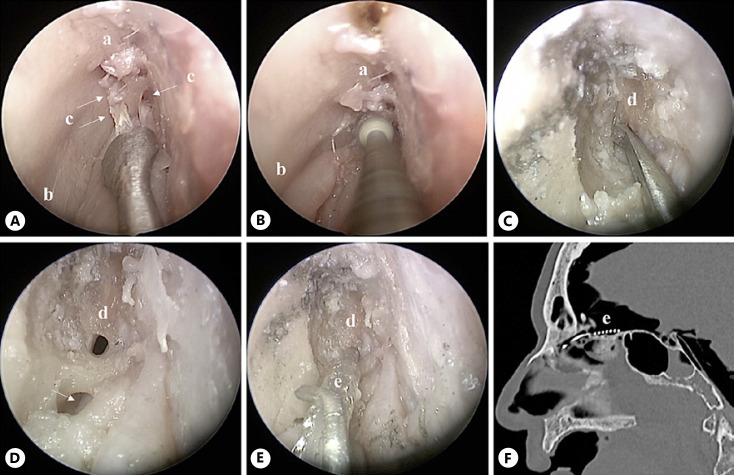
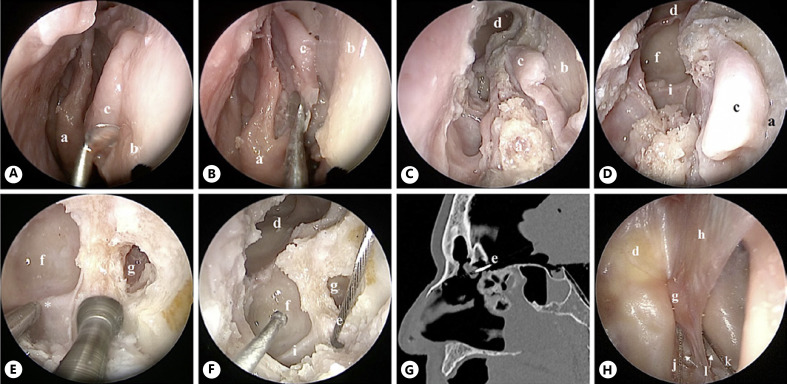
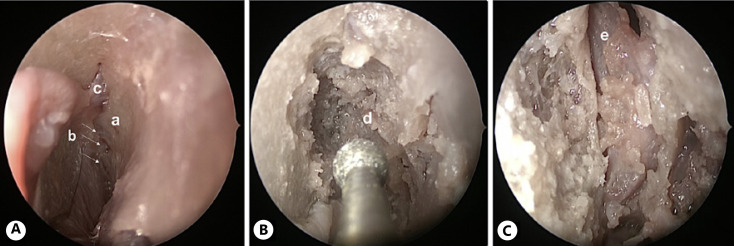
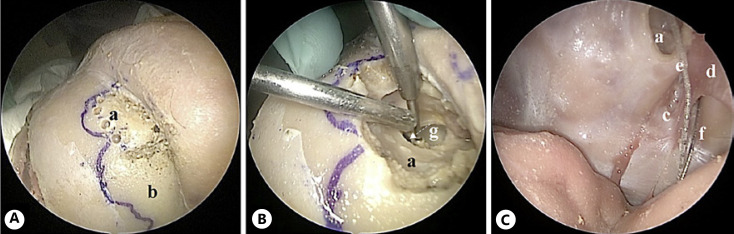
Methods: In a human anatomic cadaver study, we investigated different endoscopic approaches to electrically stimulate the olfactory bulb (OB) based on the following considerations: (1) the stimulating electrode should be close to the OB. (2) The surgical procedure should be as non-invasive and safe as possible and (3) as easy as possible for an experienced ENT surgeon.
Results: In summary, the endoscopic intracranial positioning of the electrode via a widened ostium of the fila olfactoria or a frontal sinus surgery like a Draf IIb procedure is a good option in terms of patients' risk, degree of difficulty for ENT surgeons, and position to the OB. Endoscopic intranasal positioning appeared to be the best option in terms of patient risk and the degree of difficulty for ENT surgeons. Although a bigger approach to the OB using a drill and the combined intranasal endoscopic and external approach enabled a close placement of the electrode to the OB, they do not seem relevant in practice due to their higher invasiveness.
Conclusion: The study suggested that an intranasal positioning of a stimulating electrode is possible, with placements beneath the cribriform plate, extra- or intracranially, applying elegant surgical techniques with low or medium risk to the patient and a close placement to OB.
Keywords: Olfactory dysfunction; Olfactory implant; Sinus surgery; Smell; Surgery.
© 2023 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Brämerson A, Johansson L, Ek L, Nordin S, Bende M. Prevalence of olfactory dysfunction the skövde population-based study. Laryngoscope. 2004 Apr;114((4)):733–737. - PubMed
-
- Landis BN, Konnerth CG, Hummel T. A study on the frequency of olfactory dysfunction. Laryngoscope. 2004 Oct;114((10)):1764–1769. - PubMed
-
- Vennemann MM, Hummel T, Berger K. The association between smoking and smell and taste impairment in the general population. J Neurol. 2008 Aug 28;255((8)):1121–1126. - PubMed
-
- Damm M, Temmel A, Welge-Lüssen A, Eckel HE, Kreft MP, Klussmann JP, et al. [Olfactory dysfunctions. Epidemiology and therapy in Germany, Austria and Switzerland] HNO. 2004 Feb 1;52((2)):112–120. - PubMed
-
- Desiato VM, Levy DA, Byun YJ, Nguyen SA, Soler ZM, Schlosser RJ. The prevalence of olfactory dysfunction in the general population a systematic review and meta-analysis. Am J Rhinol Allergy. 2021 Mar 1;35((2)):195–205. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
