

Digital Breast Tomosynthesis Plus Ultrasound Versus Digital Mammography Plus Ultrasound for Screening Breast Cancer in Women With Dense Breasts
- PMID: 36996902
- PMCID: PMC10067692
- DOI: 10.3348/kjr.2022.0649
Digital Breast Tomosynthesis Plus Ultrasound Versus Digital Mammography Plus Ultrasound for Screening Breast Cancer in Women With Dense Breasts
Abstract
Objective: To compare the outcomes of digital breast tomosynthesis (DBT) screening combined with ultrasound (US) with those of digital mammography (DM) combined with US in women with dense breasts.
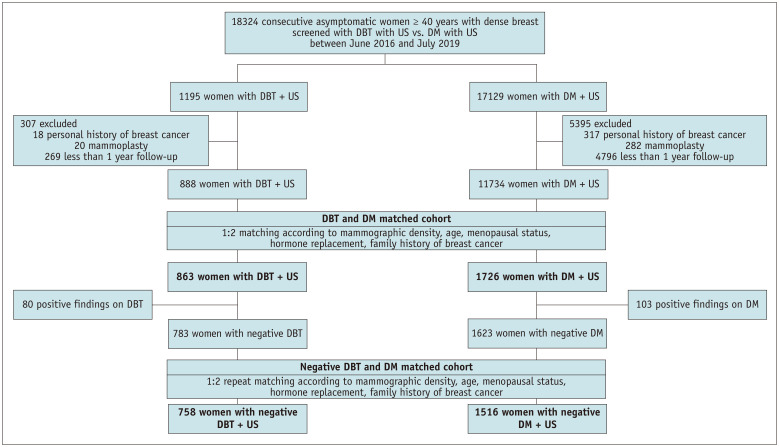
Materials and methods: A retrospective database search identified consecutive asymptomatic women with dense breasts who underwent breast cancer screening with DBT or DM and whole-breast US simultaneously between June 2016 and July 2019. Women who underwent DBT + US (DBT cohort) and DM + US (DM cohort) were matched using 1:2 ratio according to mammographic density, age, menopausal status, hormone replacement therapy, and a family history of breast cancer. The cancer detection rate (CDR) per 1000 screening examinations, abnormal interpretation rate (AIR), sensitivity, and specificity were compared.
Results: A total of 863 women in the DBT cohort were matched with 1726 women in the DM cohort (median age, 53 years; interquartile range, 40-78 years) and 26 breast cancers (9 in the DBT cohort and 17 in the DM cohort) were identified. The DBT and DM cohorts showed comparable CDR (10.4 [9 of 863; 95% confidence interval {CI}: 4.8-19.7] vs. 9.8 [17 of 1726; 95% CI: 5.7-15.7] per 1000 examinations, respectively; P = 0.889). DBT cohort showed a higher AIR than the DM cohort (31.6% [273 of 863; 95% CI: 28.5%-34.9%] vs. 22.4% [387 of 1726; 95% CI: 20.5%-24.5%]; P < 0.001). The sensitivity for both cohorts was 100%. In women with negative findings on DBT or DM, supplemental US yielded similar CDRs in both DBT and DM cohorts (4.0 vs. 3.3 per 1000 examinations, respectively; P = 0.803) and higher AIR in the DBT cohort (24.8% [188 of 758; 95% CI: 21.8%-28.0%] vs. 16.9% [257 of 1516; 95% CI: 15.1%-18.9%; P < 0.001).
Conclusion: DBT screening combined with US showed comparable CDR but lower specificity than DM screening combined with US in women with dense breasts.
Keywords: Breast cancer; Digital breast tomosynthesis; Mammography; Screening; Ultrasound.
Copyright © 2023 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Addition of Screening Breast US to Digital Mammography and Digital Breast Tomosynthesis for Breast Cancer Screening in Women at Average Risk.Radiology. 2021 Mar;298(3):568-575. doi: 10.1148/radiol.2021203134. Epub 2021 Jan 12. Radiology. 2021. PMID: 33434108
-
Screening Performance of Digital Breast Tomosynthesis vs Digital Mammography in Community Practice by Patient Age, Screening Round, and Breast Density.JAMA Netw Open. 2020 Jul 1;3(7):e2011792. doi: 10.1001/jamanetworkopen.2020.11792. JAMA Netw Open. 2020. PMID: 32721031 Free PMC article.
-
Association of Digital Breast Tomosynthesis vs Digital Mammography With Cancer Detection and Recall Rates by Age and Breast Density.JAMA Oncol. 2019 May 1;5(5):635-642. doi: 10.1001/jamaoncol.2018.7078. JAMA Oncol. 2019. PMID: 30816931 Free PMC article.
-
Digital Breast Tomosynthesis with Hologic 3D Mammography Selenia Dimensions System for Use in Breast Cancer Screening: A Single Technology Assessment [Internet].Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Sep 4. Report from the Norwegian Institute of Public Health No. 2017-08. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Sep 4. Report from the Norwegian Institute of Public Health No. 2017-08. PMID: 29553669 Free Books & Documents. Review.
-
Digital breast tomosynthesis for breast cancer screening and diagnosis in women with dense breasts - a systematic review and meta-analysis.BMC Cancer. 2018 Apr 3;18(1):380. doi: 10.1186/s12885-018-4263-3. BMC Cancer. 2018. PMID: 29615072 Free PMC article.
Cited by
-
Breast Cancer Screening in Asian Countries: Epidemiology, Screening Practices, Outcomes, Challenges, and Future Directions.Korean J Radiol. 2025 Aug;26(8):743-758. doi: 10.3348/kjr.2025.0338. Korean J Radiol. 2025. PMID: 40736408 Free PMC article. Review.
-
Comparative Diagnostic Efficacy of Four Breast Imaging Modalities in Dense Breasts: A Single-Center Retrospective Study.Biomedicines. 2025 Jul 17;13(7):1750. doi: 10.3390/biomedicines13071750. Biomedicines. 2025. PMID: 40722820 Free PMC article.
-
Downgrading Breast Imaging Reporting and Data System categories in ultrasound using strain elastography and computer-aided diagnosis system: a multicenter, prospective study.Br J Radiol. 2024 Oct 1;97(1162):1653-1660. doi: 10.1093/bjr/tqae136. Br J Radiol. 2024. PMID: 39102827 Free PMC article.
References
-
- Nelson HD, Fu R, Cantor A, Pappas M, Daeges M, Humphrey L. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 U.S. Preventive Services Task Force recommendation. Ann Intern Med. 2016;164:244–255. - PubMed
-
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225:165–175. - PubMed
-
- Buchberger W, Geiger-Gritsch S, Knapp R, Gautsch K, Oberaigner W. Combined screening with mammography and ultrasound in a population-based screening program. Eur J Radiol. 2018;101:24–29. - PubMed
-
- Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356:227–236. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
