

A biomarker for bacteremia in pregnant women with acute pyelonephritis: soluble suppressor of tumorigenicity 2 or sST2
- PMID: 36997168
- PMCID: PMC10352993
- DOI: 10.1080/14767058.2023.2183470
A biomarker for bacteremia in pregnant women with acute pyelonephritis: soluble suppressor of tumorigenicity 2 or sST2
Abstract
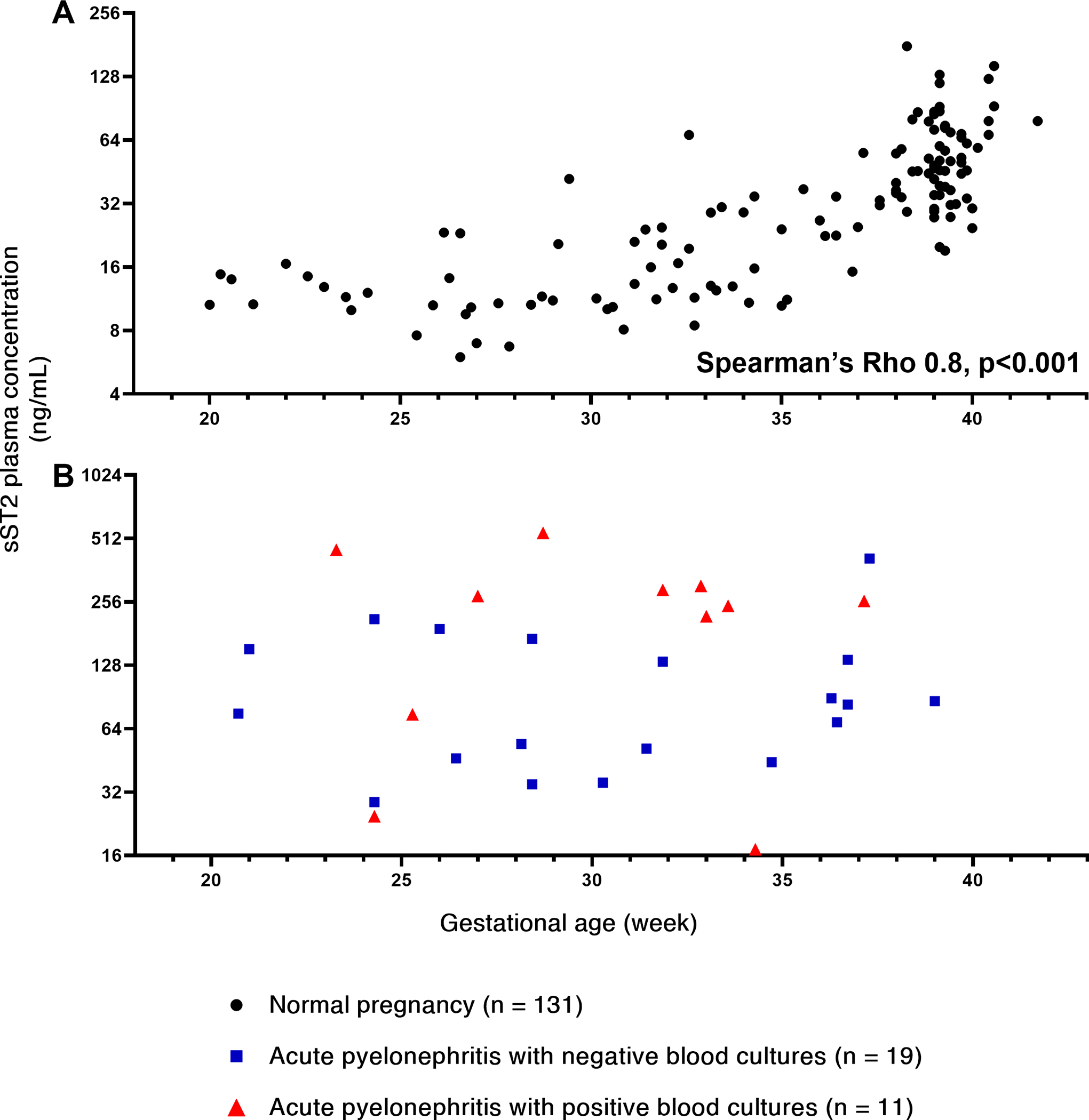
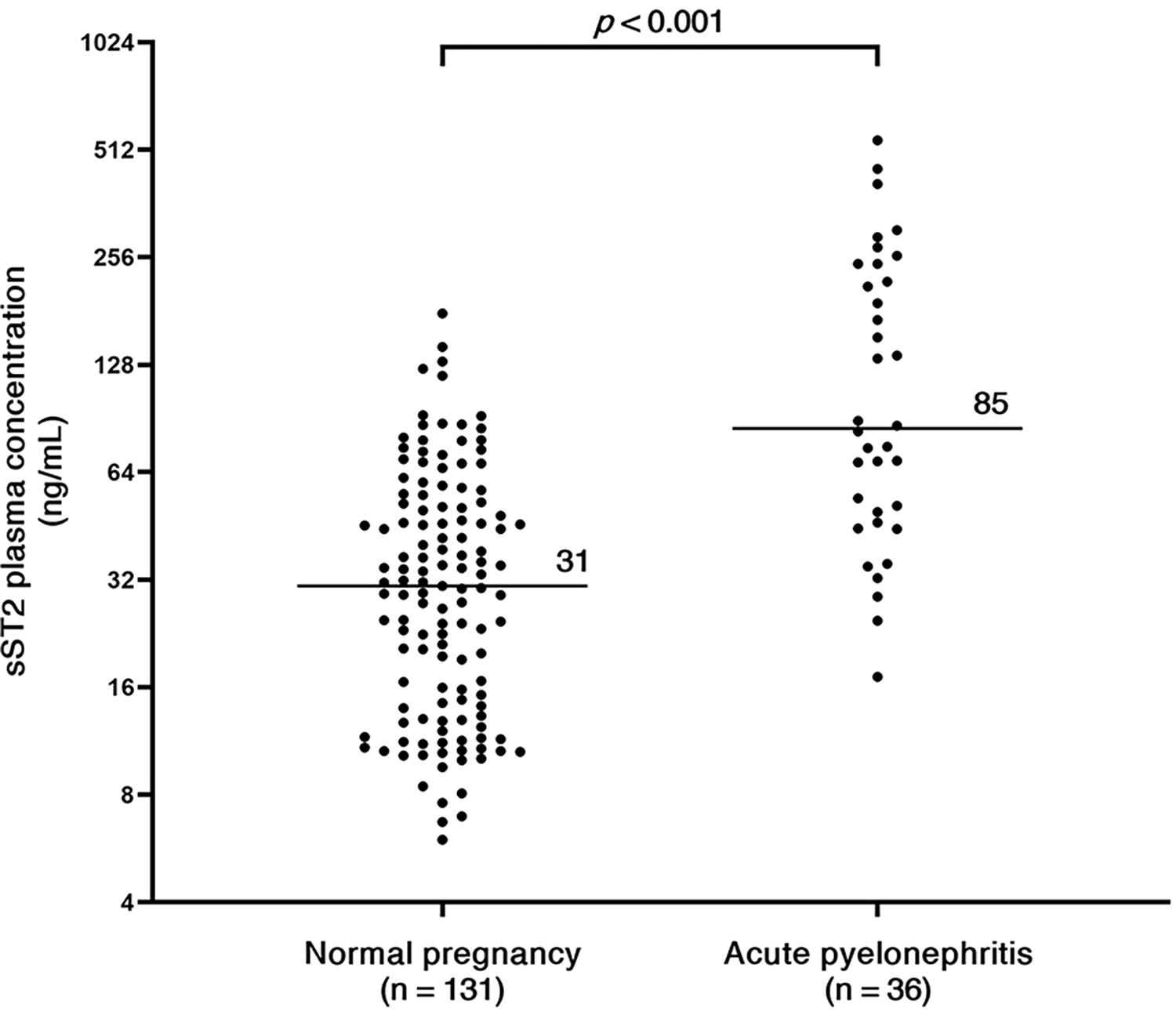
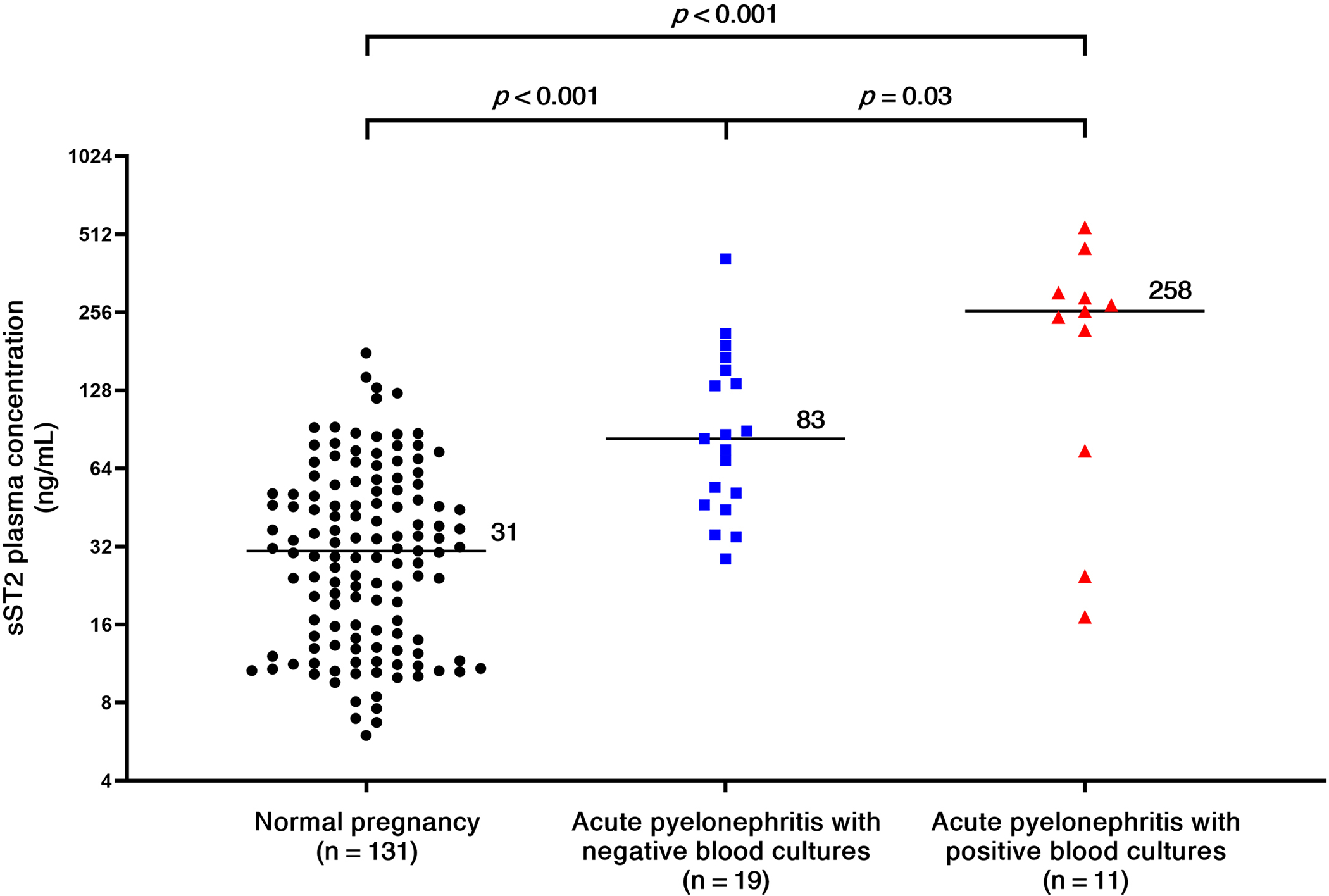
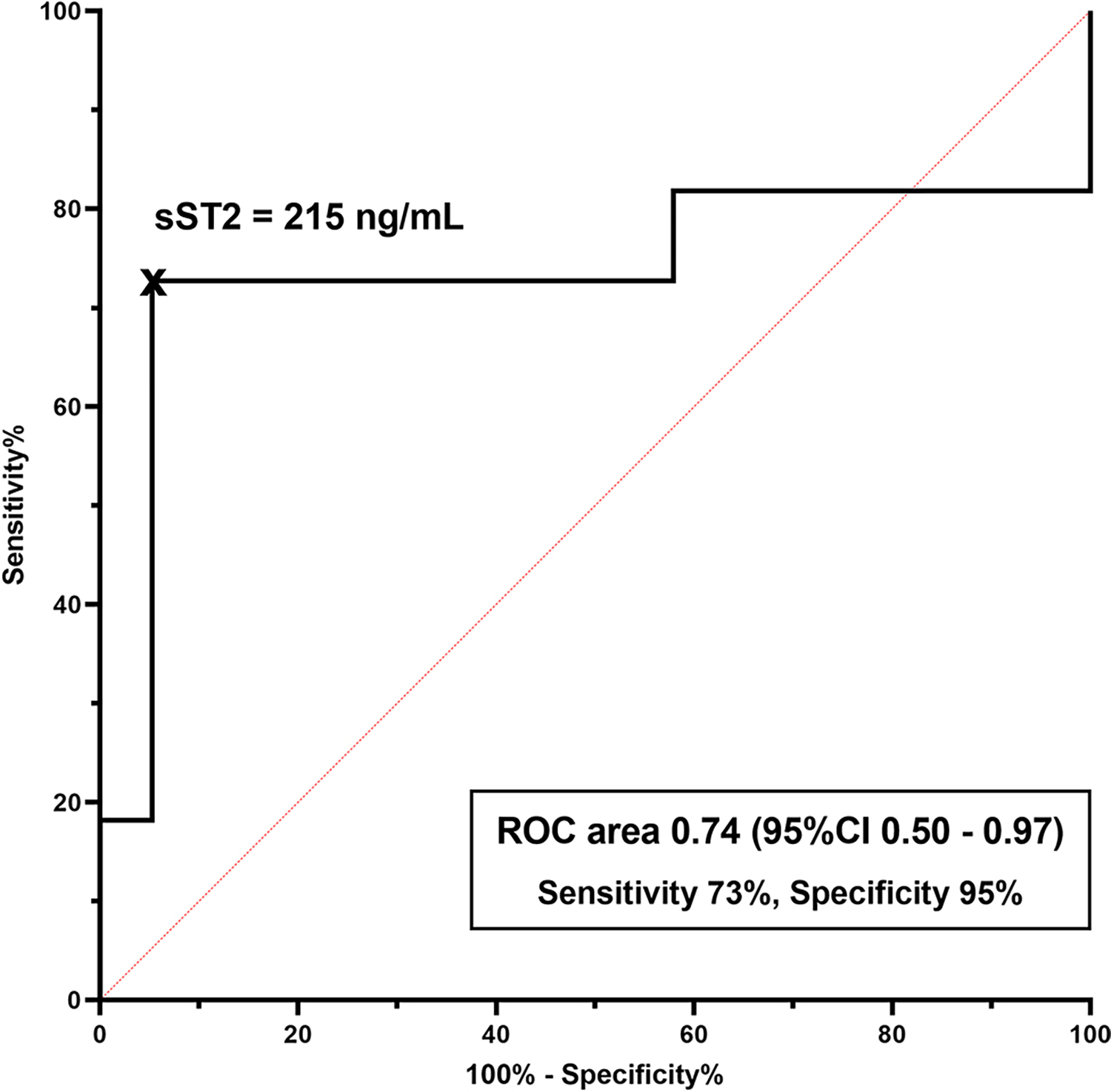
Objective: Sepsis is a leading cause of maternal death, and its diagnosis during the golden hour is critical to improve survival. Acute pyelonephritis in pregnancy is a risk factor for obstetrical and medical complications, and it is a major cause of sepsis, as bacteremia complicates 15-20% of pyelonephritis episodes in pregnancy. The diagnosis of bacteremia currently relies on blood cultures, whereas a rapid test could allow timely management and improved outcomes. Soluble suppression of tumorigenicity 2 (sST2) was previously proposed as a biomarker for sepsis in non-pregnant adults and children. This study was designed to determine whether maternal plasma concentrations of sST2 in pregnant patients with pyelonephritis can help to identify those at risk for bacteremia.Study design: This cross-sectional study included women with normal pregnancy (n = 131) and pregnant women with acute pyelonephritis (n = 36). Acute pyelonephritis was diagnosed based on a combination of clinical findings and a positive urine culture. Patients were further classified according to the results of blood cultures into those with and without bacteremia. Plasma concentrations of sST2 were determined by a sensitive immunoassay. Non-parametric statistics were used for analysis.Results: The maternal plasma sST2 concentration increased with gestational age in normal pregnancies. Pregnant patients with acute pyelonephritis had a higher median (interquartile range) plasma sST2 concentration than those with a normal pregnancy [85 (47-239) ng/mL vs. 31 (14-52) ng/mL, p < .001]. Among patients with pyelonephritis, those with a positive blood culture had a median plasma concentration of sST2 higher than that of patients with a negative blood culture [258 (IQR: 75-305) ng/mL vs. 83 (IQR: 46-153) ng/mL; p = .03]. An elevated plasma concentration of sST2 ≥ 215 ng/mL had a sensitivity of 73% and a specificity of 95% (area under the receiver operating characteristic curve, 0.74; p = .003) with a positive likelihood ratio of 13.8 and a negative likelihood ratio of 0.3 for the identification of patients who had a positive blood culture.Conclusion: sST2 is a candidate biomarker to identify bacteremia in pregnant women with pyelonephritis. Rapid identification of these patients may optimize patient care.
Keywords: Cytokines; IL-1; IL-33; pregnancy; sepsis; septic shock; urinary tract infection.
Conflict of interest statement
Figures
Similar articles
-
Acute pyelonephritis in pregnancy and plasma syndecan-1: evidence of glycocalyx involvement.J Matern Fetal Neonatal Med. 2023 Dec;36(1):2155041. doi: 10.1080/14767058.2022.2155041. J Matern Fetal Neonatal Med. 2023. PMID: 36642424 Free PMC article.
-
Endocan, a putative endothelial cell marker, is elevated in preeclampsia, decreased in acute pyelonephritis, and unchanged in other obstetrical syndromes.J Matern Fetal Neonatal Med. 2015;28(14):1621-32. doi: 10.3109/14767058.2014.964676. Epub 2014 Oct 28. J Matern Fetal Neonatal Med. 2015. PMID: 25211383 Free PMC article.
-
Maternal serum soluble CD30 is increased in pregnancies complicated with acute pyelonephritis.J Matern Fetal Neonatal Med. 2007 Nov;20(11):803-11. doi: 10.1080/14767050701492851. J Matern Fetal Neonatal Med. 2007. PMID: 17853184 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Best Clinical Practice: Blood Culture Utility in the Emergency Department.J Emerg Med. 2016 Nov;51(5):529-539. doi: 10.1016/j.jemermed.2016.07.003. Epub 2016 Sep 14. J Emerg Med. 2016. PMID: 27639424 Review.
References
-
- Cunningham FG, Morris GB, Mickal A. Acute pyelonephritis of pregnancy: A clinical review. Obstetrics and gynecology 1973;42:112–7. - PubMed
-
- Gilstrap LC 3rd, Cunningham FG, Whalley PJ. Acute pyelonephritis in pregnancy: an anterospective study. Obstetrics and gynecology 1981;57:409–13. - PubMed
-
- Sheffield JS, Cunningham FG. Urinary tract infection in women. Obstetrics and gynecology 2005;106:1085–92. - PubMed
-
- Wing DA, Fassett MJ, Getahun D. Acute pyelonephritis in pregnancy: an 18-year retrospective analysis. American journal of obstetrics and gynecology 2014;210:219.e1–6. - PubMed
-
- Cunningham FG, Lucas MJ, Hankins GD. Pulmonary injury complicating antepartum pyelonephritis. American journal of obstetrics and gynecology 1987;156:797–807. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources