

A multi-institutional study using artificial intelligence to provide reliable and fair feedback to surgeons
- PMID: 36997578
- PMCID: PMC10063640
- DOI: 10.1038/s43856-023-00263-3
A multi-institutional study using artificial intelligence to provide reliable and fair feedback to surgeons
Abstract
Background: Surgeons who receive reliable feedback on their performance quickly master the skills necessary for surgery. Such performance-based feedback can be provided by a recently-developed artificial intelligence (AI) system that assesses a surgeon's skills based on a surgical video while simultaneously highlighting aspects of the video most pertinent to the assessment. However, it remains an open question whether these highlights, or explanations, are equally reliable for all surgeons.
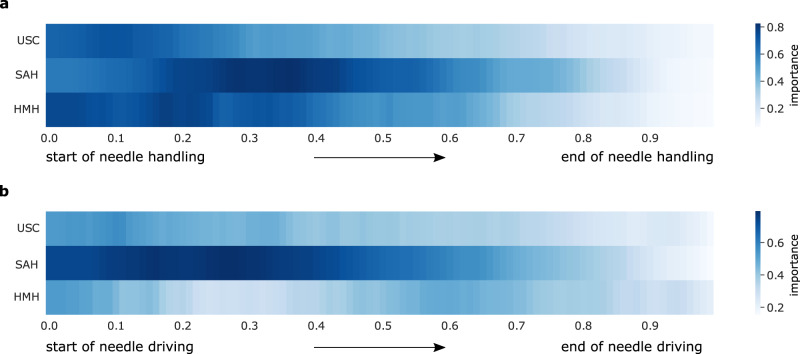
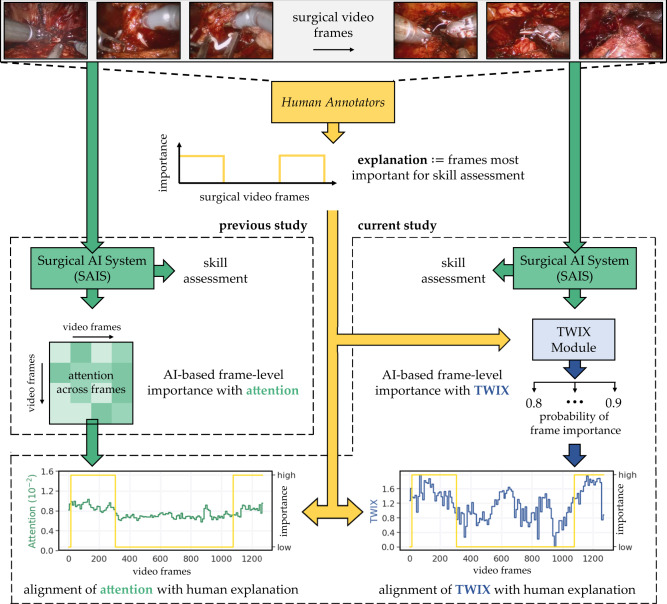
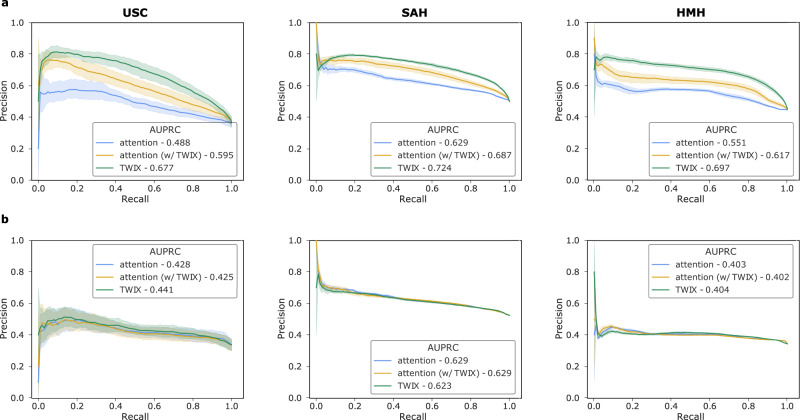
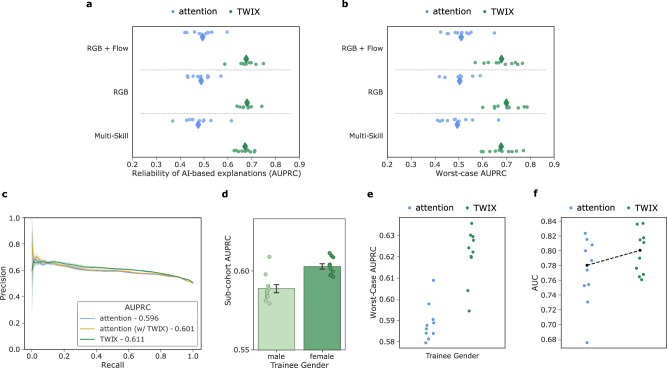
Methods: Here, we systematically quantify the reliability of AI-based explanations on surgical videos from three hospitals across two continents by comparing them to explanations generated by humans experts. To improve the reliability of AI-based explanations, we propose the strategy of training with explanations -TWIX -which uses human explanations as supervision to explicitly teach an AI system to highlight important video frames.
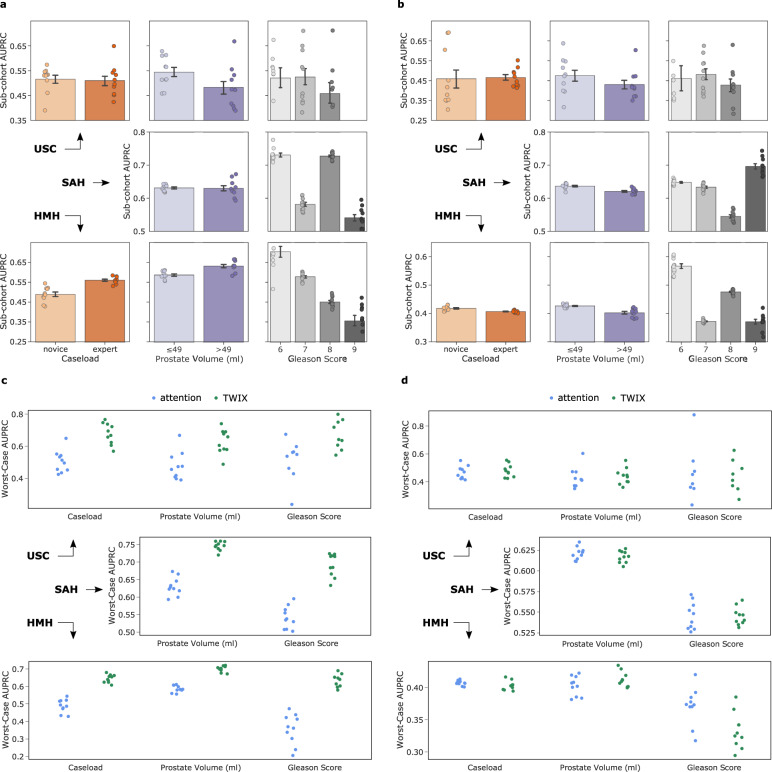
Results: We show that while AI-based explanations often align with human explanations, they are not equally reliable for different sub-cohorts of surgeons (e.g., novices vs. experts), a phenomenon we refer to as an explanation bias. We also show that TWIX enhances the reliability of AI-based explanations, mitigates the explanation bias, and improves the performance of AI systems across hospitals. These findings extend to a training environment where medical students can be provided with feedback today.
Conclusions: Our study informs the impending implementation of AI-augmented surgical training and surgeon credentialing programs, and contributes to the safe and fair democratization of surgery.
Plain language summary
Surgeons aim to master skills necessary for surgery. One such skill is suturing which involves connecting objects together through a series of stitches. Mastering these surgical skills can be improved by providing surgeons with feedback on the quality of their performance. However, such feedback is often absent from surgical practice. Although performance-based feedback can be provided, in theory, by recently-developed artificial intelligence (AI) systems that use a computational model to assess a surgeon’s skill, the reliability of this feedback remains unknown. Here, we compare AI-based feedback to that provided by human experts and demonstrate that they often overlap with one another. We also show that explicitly teaching an AI system to align with human feedback further improves the reliability of AI-based feedback on new videos of surgery. Our findings outline the potential of AI systems to support the training of surgeons by providing feedback that is reliable and focused on a particular skill, and guide programs that give surgeons qualifications by complementing skill assessments with explanations that increase the trustworthiness of such assessments.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: D.K. is a paid consultant of Flatiron Health and an employee of Vicarious Surgical. C.W. is a paid consultant of Intuitive Surgical. A.A. is an employee of Nvidia. A.J.H is a consultant of Intuitive Surgical. The remaining authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
