

Continuous cuffless blood pressure monitoring with a wearable ring bioimpedance device
- PMID: 36997608
- PMCID: PMC10063561
- DOI: 10.1038/s41746-023-00796-w
Continuous cuffless blood pressure monitoring with a wearable ring bioimpedance device
Abstract
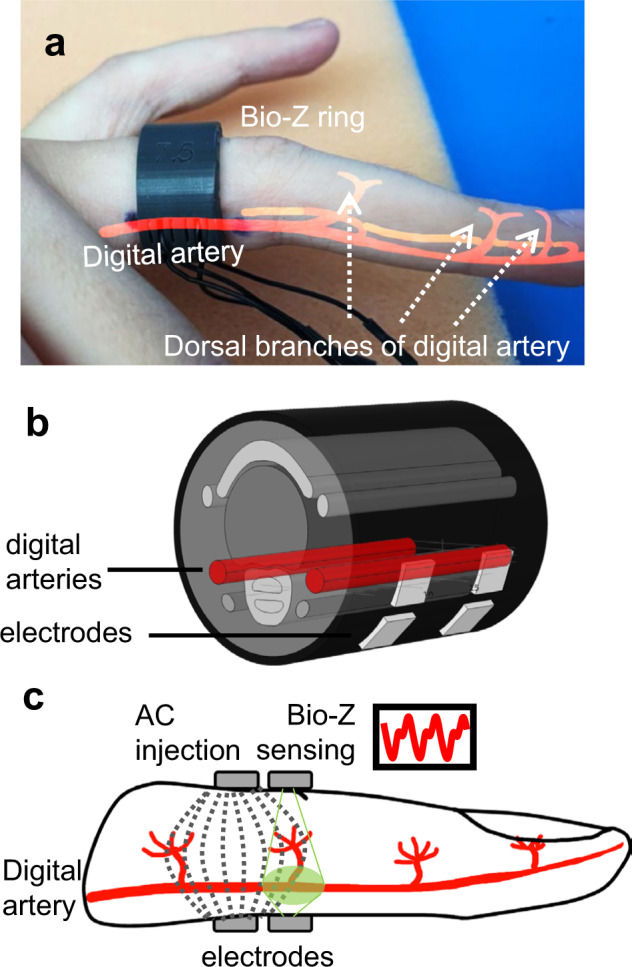
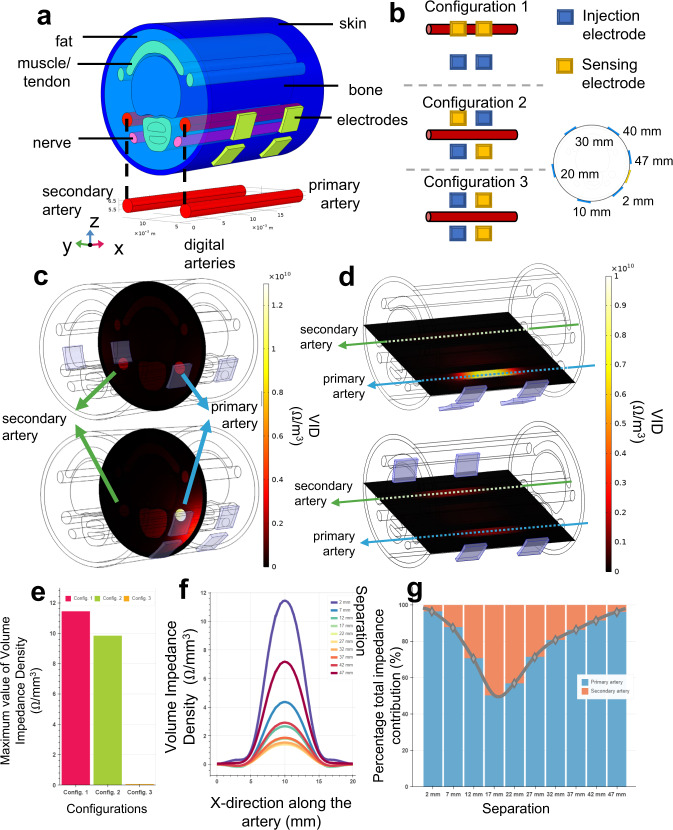
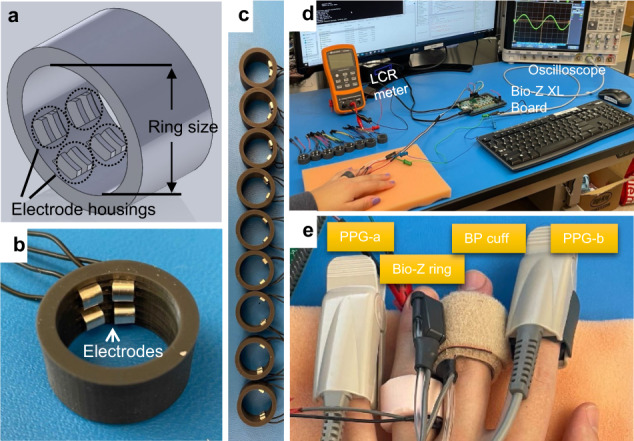
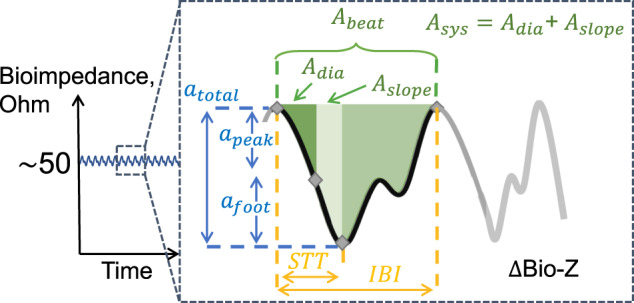
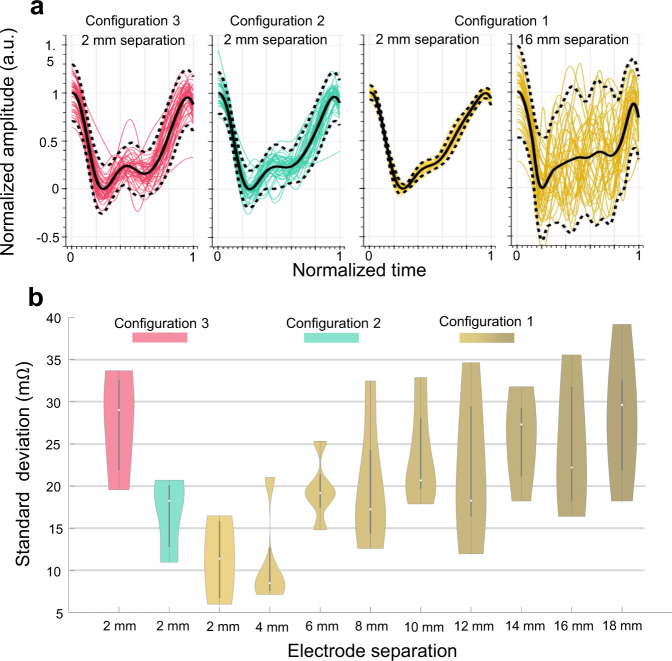
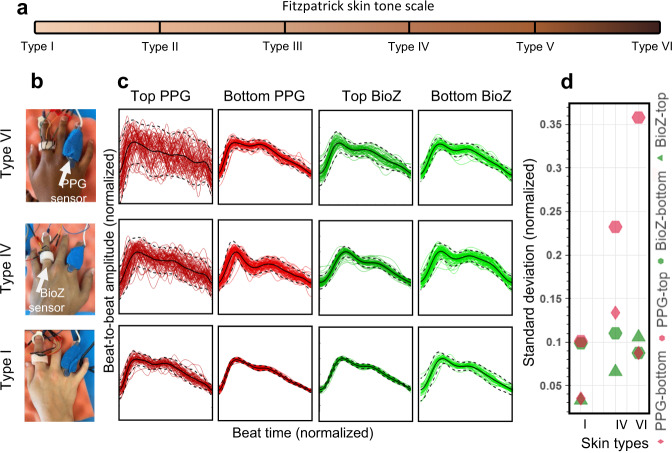
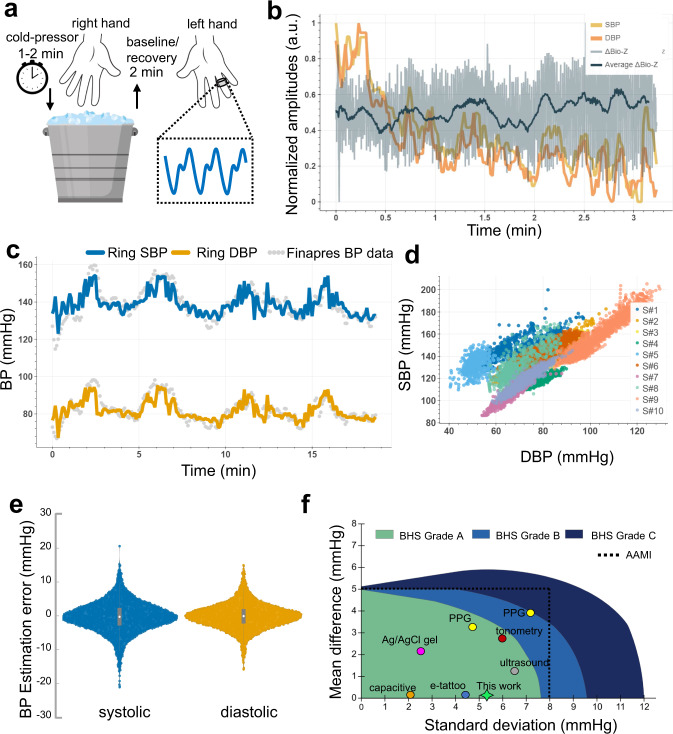
Smart rings provide unique opportunities for continuous physiological measurement. They are easy to wear, provide little burden in comparison to other smart wearables, are suitable for nocturnal settings, and can be sized to provide ideal contact between the sensors and the skin at all times. Continuous measuring of blood pressure (BP) provides essential diagnostic and prognostic value for cardiovascular health management. However, conventional ambulatory BP measurement devices operate using an inflating cuff that is bulky, intrusive, and impractical for frequent or continuous measurements. We introduce ring-shaped bioimpedance sensors leveraging the deep tissue sensing ability of bioimpedance while introducing no sensitivity to skin tones, unlike optical modalities. We integrate unique human finger finite element model with exhaustive experimental data from participants and derive optimum design parameters for electrode placement and sizes that yields highest sensitivity to arterial volumetric changes, with no discrimination against varying skin tones. BP is constructed using machine learning algorithms. The ring sensors are used to estimate arterial BP showing peak correlations of 0.81, and low error (systolic BP: 0.11 ± 5.27 mmHg, diastolic BP: 0.11 ± 3.87 mmHg) for >2000 data points and wide BP ranges (systolic: 89-213 mmHg and diastolic: 42-122 mmHg), highlighting the significant potential use of bioimpedance ring for accurate and continuous estimation of BP.
© 2023. The Author(s).
Conflict of interest statement
R.J. is an Associate Editor of
Figures

References
Grants and funding
- 1R01HL151240/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- 1R01HL151240/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- 1R01EB028106/U.S. Department of Health & Human Services | NIH | National Institute of Biomedical Imaging and Bioengineering (NIBIB)
- 1R01EB028106/U.S. Department of Health & Human Services | NIH | National Institute of Biomedical Imaging and Bioengineering (NIBIB)
LinkOut - more resources
Full Text Sources
Other Literature Sources
