

Investigating rapid diagnostic testing in Kenya's health system, 2018-2020: validating non-reporting in routine data using a health facility service assessment survey
- PMID: 36997953
- PMCID: PMC10061357
- DOI: 10.1186/s12913-023-09296-9
Investigating rapid diagnostic testing in Kenya's health system, 2018-2020: validating non-reporting in routine data using a health facility service assessment survey
Abstract
Background: Understanding the availability of rapid diagnostic tests (RDTs) is essential for attaining universal health care and reducing health inequalities. Although routine data helps measure RDT coverage and health access gaps, many healthcare facilities fail to report their monthly diagnostic test data to routine health systems, impacting routine data quality. This study sought to understand whether non-reporting by facilities is due to a lack of diagnostic and/or service provision capacity by triangulating routine and health service assessment survey data in Kenya.
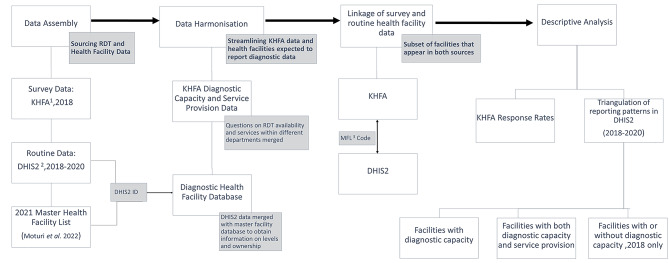
Methods: Routine facility-level data on RDT administration were sourced from the Kenya health information system for the years 2018-2020. Data on diagnostic capacity (RDT availability) and service provision (screening, diagnosis, and treatment) were obtained from a national health facility assessment conducted in 2018. The two sources were linked and compared obtaining information on 10 RDTs from both sources. The study then assessed reporting in the routine system among facilities with (i) diagnostic capacity only, (ii) both confirmed diagnostic capacity and service provision and (iii) without diagnostic capacity. Analyses were conducted nationally, disaggregated by RDT, facility level and ownership.
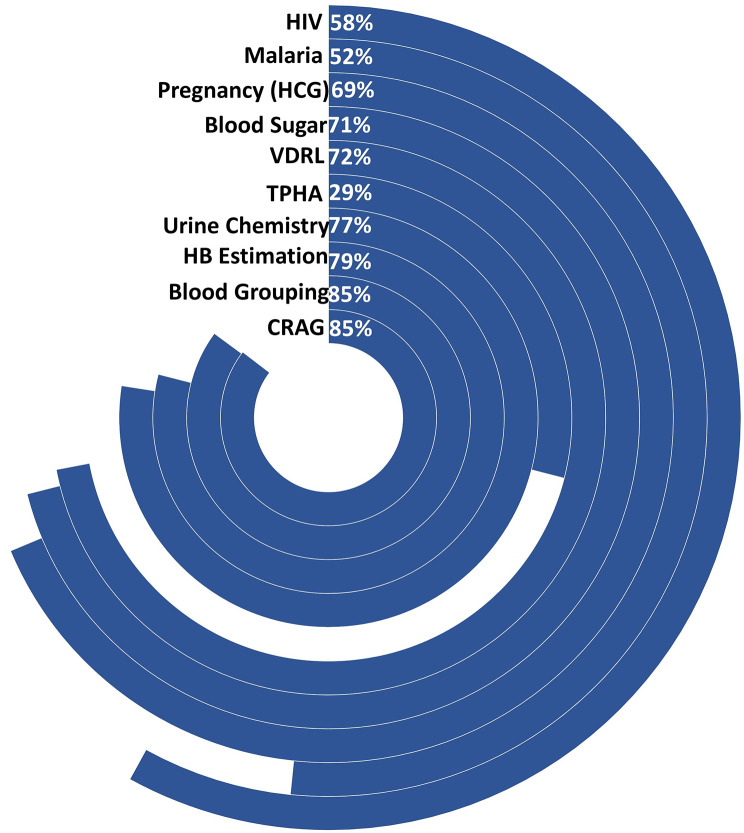
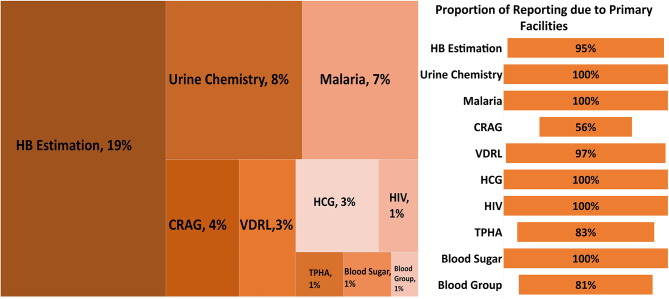
Results: Twenty-one per cent (2821) of all facilities expected to report routine diagnostic data in Kenya were included in the triangulation. Most (86%) were primary-level facilities under public ownership (70%). Overall, survey response rates on diagnostic capacity were high (> 70%). Malaria and HIV had the highest response rate (> 96%) and the broadest coverage in diagnostic capacity across facilities (> 76%). Reporting among facilities with diagnostic capacity varied by test, with HIV and malaria having the lowest reporting rates, 58% and 52%, respectively, while the rest ranged between 69% and 85%. Among facilities with both service provision and diagnostic capacity, reporting ranged between 52% and 83% across tests. Public and secondary facilities had the highest reporting rates across all tests. A small proportion of health facilities without diagnostic capacity submitted testing reports in 2018, most of which were primary facilities.
Conclusion: Non-reporting in routine health systems is not always due to a lack of capacity. Further analyses are required to inform other drivers of non-reporting to ensure reliable routine health data.
Keywords: Health facility survey; Kenya; Rapid diagnostic test; Routine data; Triangulation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Catharina B, Madhukar P. Diagnostic Gaps in Global Health. https://www.thinkglobalhealth.org/article/diagnostic-gaps-global-health. Accessed August 2022.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
