

The impact of impaired sleep quality on symptom change and future exacerbation of chronic obstructive pulmonary disease
- PMID: 36998013
- PMCID: PMC10064786
- DOI: 10.1186/s12931-023-02405-6
The impact of impaired sleep quality on symptom change and future exacerbation of chronic obstructive pulmonary disease
Abstract
Purpose: Study the impact of impaired sleep quality on symptom change and future exacerbation of chronic obstructive pulmonary disease (COPD) patients.
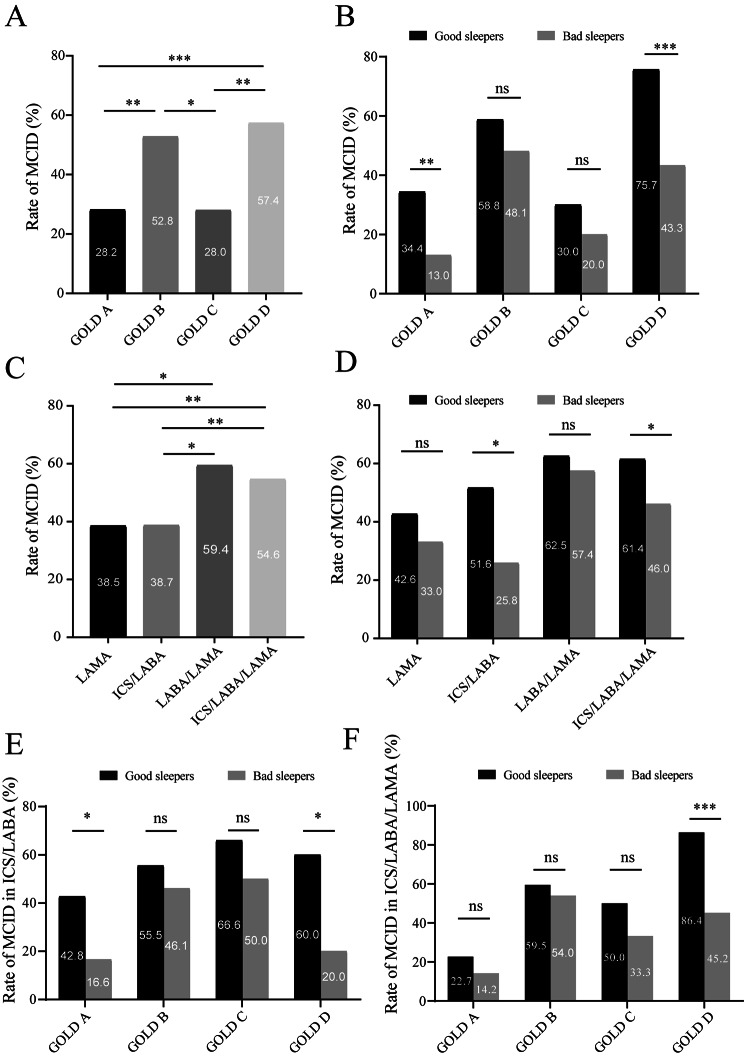
Methods: This was a prospective study. Patients with COPD were recruited into the study and followed up for one year. Pittsburgh sleep quality index (PSQI) was collected at baseline. Symptom change was assessed with Minimum clinically important difference (MCID) in COPD Assessment Test (CAT) at 6-month visit, which is an indicator to assess symptom improvement. Exacerbation was recorded during the one-year visit. PSQI score > 5 was defined as poor sleep quality, whereas PSQI score ≤ 5 was defined as good sleep quality. MCID was defined as attaining a CAT decrease ≥ 2.
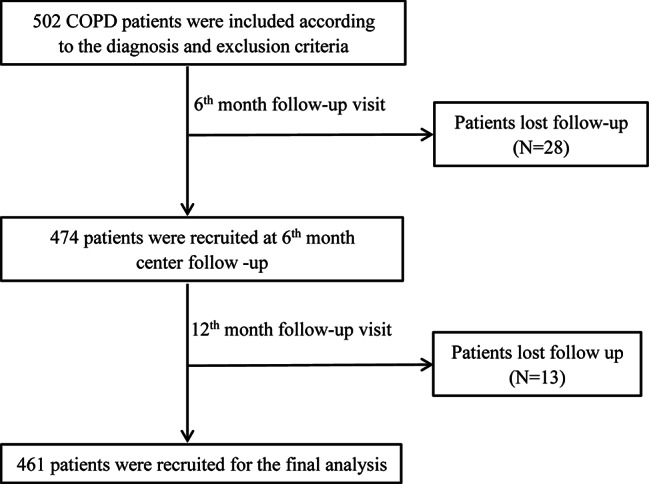
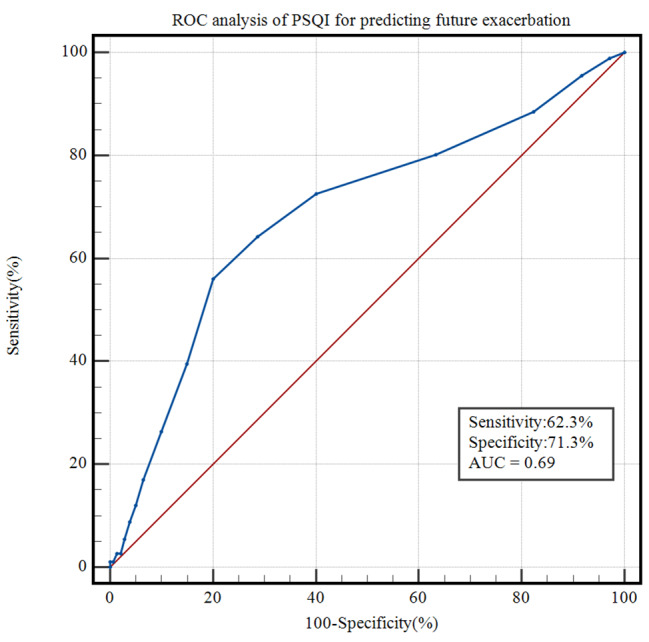
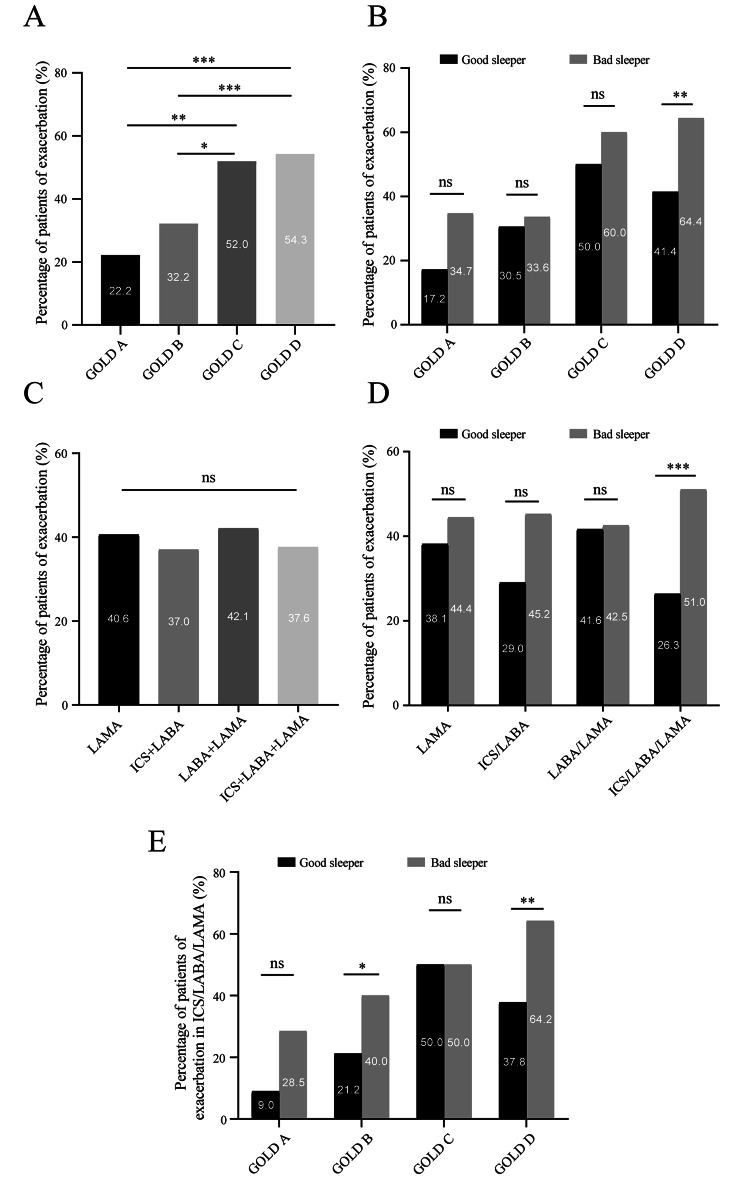
Results: A total of 461 patients were enrolled for final analysis. Two hundred twenty-eight (49.4%) patients had poor sleep quality. Overall, 224 (48.6%) patients attained MCID at 6-month visit and the incidence of exacerbation during the one-year visit was 39.3%. Fewer patients with impaired sleep quality achieved MCID than patients with good sleep quality. Good sleepers were significantly more likely to attain MCID (OR: 3.112, p < 0.001) than poor sleepers. Fewer poor sleepers in GOLD A and D groups attained MCID with ICS/LABA, and fewer poor sleepers in the GOLD D group attained MCID with ICS/LABA/LAMA than good sleepers. Poor sleep quality was a greater risk factor of future exacerbation in Cox regression analysis. The ROC curves showed that PSQI score had a predictive capacity for future exacerbation. More patients with poor sleep quality experienced future exacerbation in GOLD B and D group with treatment of ICS/LABA/LAMA compared to good sleepers.
Conclusions: COPD patients with impaired sleep quality were less likely to achieve symptom improvement and were at increased risk of future exacerbation compared to patients with good sleep quality. Besides, sleep disturbance may affect the symptom improvement and future exacerbation of patients with different inhaled medication or in different GOLD groups.
Keywords: COPD; Exacerbation; Sleep quality; Symptom change.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
