

Intraoperative MRI-derived volumetric ablation margins and initial correlation with local outcome after MRI-guided cryoablation of renal tumors
- PMID: 36998028
- PMCID: PMC10064595
- DOI: 10.1186/s40644-023-00546-x
Intraoperative MRI-derived volumetric ablation margins and initial correlation with local outcome after MRI-guided cryoablation of renal tumors
Abstract
Purpose: To assess volumetric ablation margins derived from intraoperative pre- and post-ablation MRI after magnetic resonance imaging (MRI)-guided percutaneous cryoablation of renal tumors and explore its correlation with local treatment success.
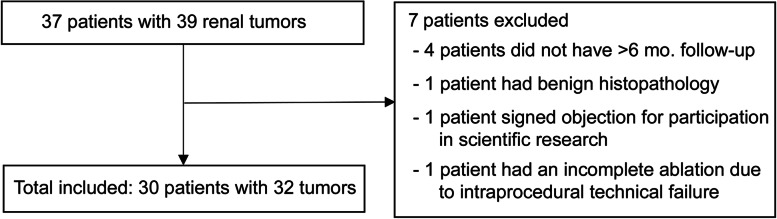
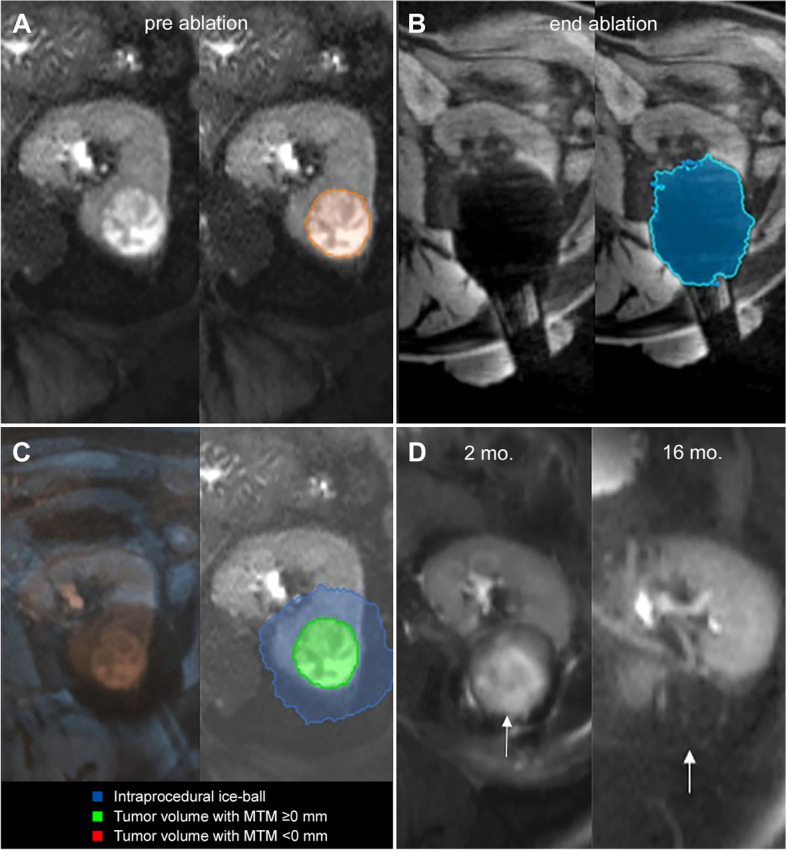
Methods: Retrospective analysis was performed on 30 patients (mean age 69y) who underwent percutaneous MRI-guided cryoablation between May 2014 and May 2020 for 32 renal tumors (size: 1.6-5.1 cm). Tumor and ice-ball volumes were segmented on intraprocedural pre- and post-ablation MR images using Software Assistant for Interventional Radiology (SAFIR) software. After MRI-MRI co-registration, the software automatically quantified the minimal treatment margin (MTM),defined as the smallest 3D distance between the tumor and ice-ball surface. Local tumor progression (LTP) after cryoablation was assessed on follow-up imaging.
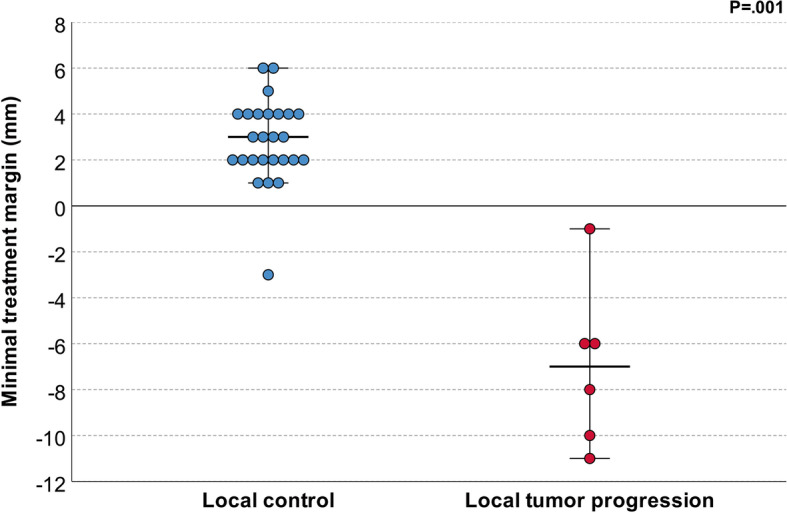
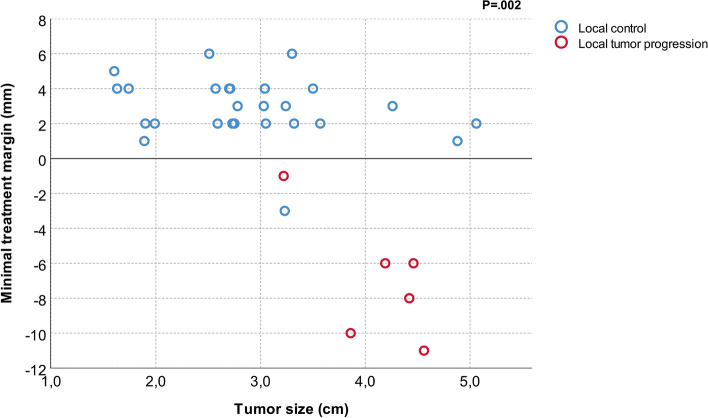
Results: Median follow-up was 16 months (range: 1-58). Local control after cryoablation was achieved in 26 cases (81%) while LTP occurred in 6 (19%). The intended MTM of ≥5 mm was achieved in 3/32 (9%) cases. Median MTM was significantly smaller for cases with (- 7 mm; IQR:-10 to - 5) vs. without LTP (3 mm; IQR:2 to 4) (P < .001). All cases of LTP had a negative MTM. All negative treatment margins occurred in tumors > 3 cm.
Conclusions: Determination of volumetric ablation margins from intraoperative MRI was feasible and may be useful in predicting local outcome after MRI-guided renal cryoablation. In our preliminary data, an intraoperative MRI-derived minimal margin extending at least 1 mm beyond the MRI-visible tumor led to local control and this was more difficult to achieve in tumors > 3 cm. Ultimately, online margin analysis may be a valuable tool to intraoperatively assess therapy success, but larger prospective studies are needed to establish a reliable threshold for clinical use.
Keywords: Local recurrence; MRI; Percutaneous cryoablation; Renal tumor; Treatment margin.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
