

Diagnostic and Management Strategies of Bietti Crystalline Dystrophy: Current Perspectives
- PMID: 36998515
- PMCID: PMC10046287
- DOI: 10.2147/OPTH.S388292
Diagnostic and Management Strategies of Bietti Crystalline Dystrophy: Current Perspectives
Abstract
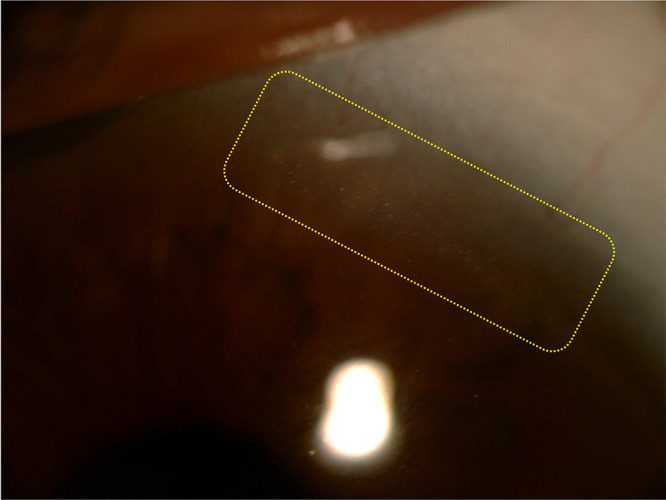
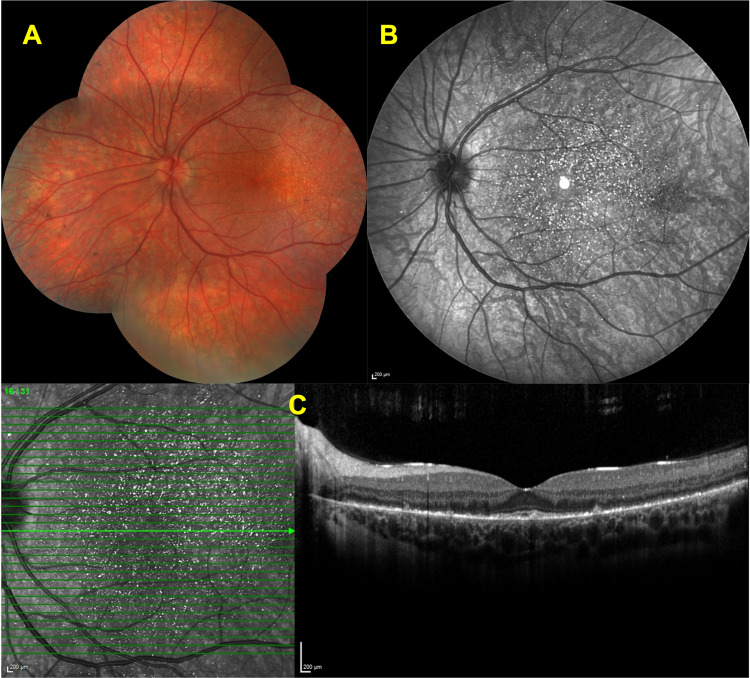
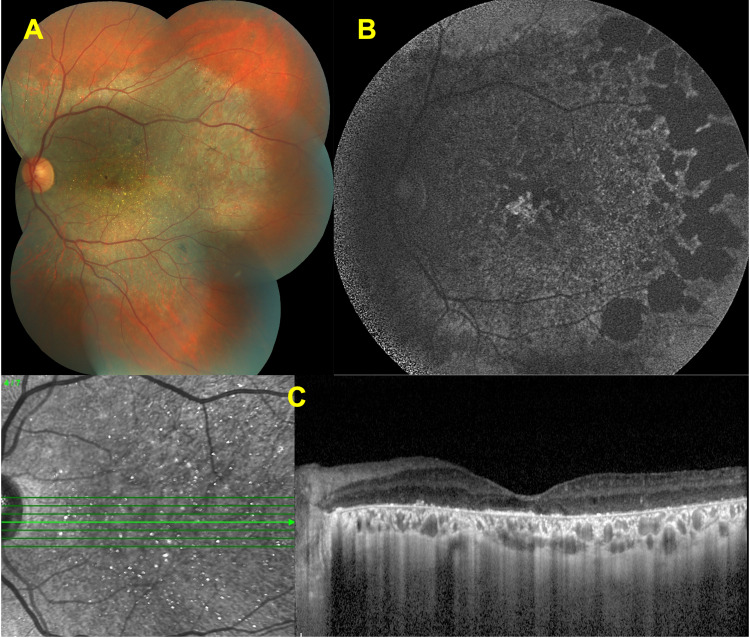
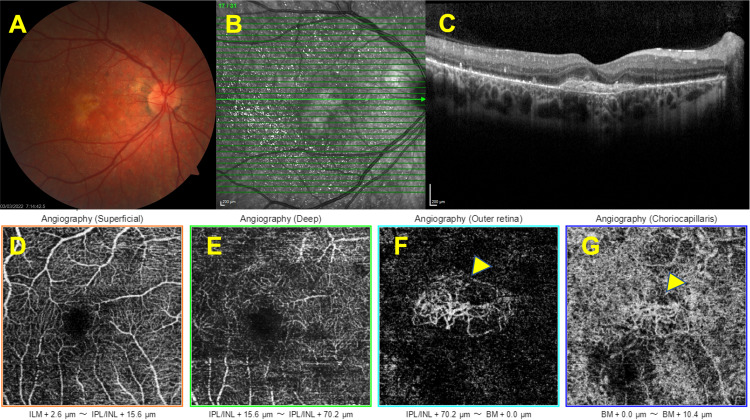
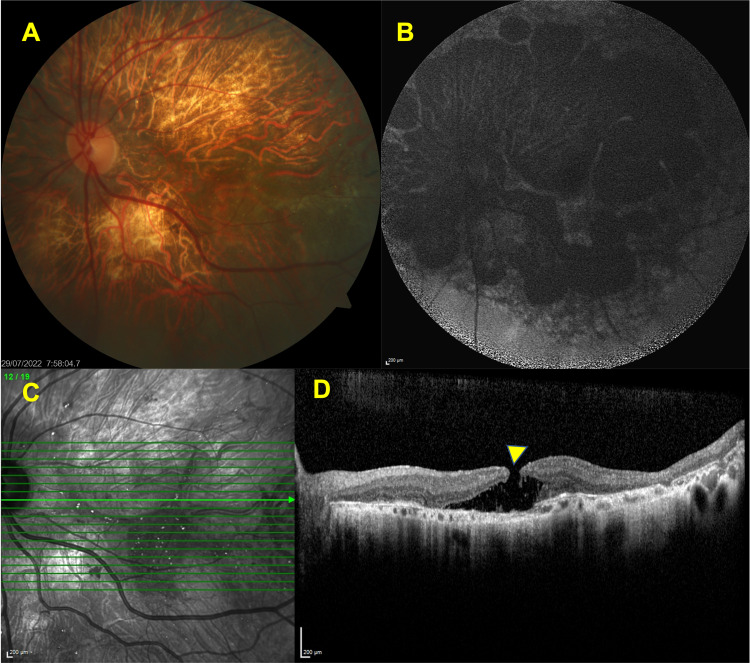
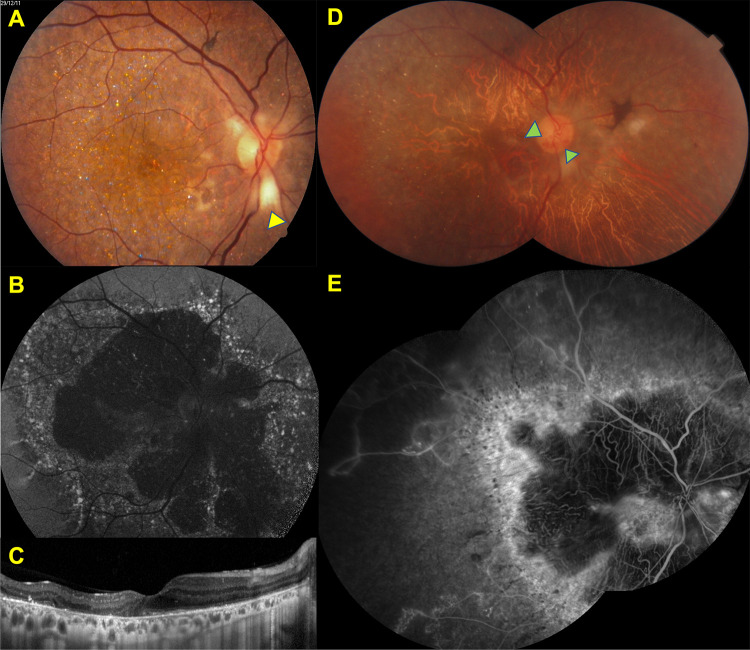
Bietti crystalline dystrophy (BCD) is a rare, genetically determined chorioretinal dystrophy presenting with intraretinal crystalline deposits and varying degrees of progressive chorioretinal atrophy commencing at the posterior pole. In some cases, there can be concomitant corneal crystals noted first in the superior or inferior limbus. CYP4V2 gene, a member of the cytochrome P450 family is responsible for the disease and more than 100 mutations have been defined thus far. However, a genotype-phenotype correlation has not been established yet. Visual impairment commonly occurs between the second and third decades of life. By the fifth or sixth decade of life, vision loss can become so severe that the patient may potentially become legally blind. Multitudes of multimodal imaging modalities can be utilized to demonstrate the clinical features, course, and complications of the disease. This present review aims to reiterate the clinical features of BCD, update the clinical perspectives with the help of multimodal imaging techniques, and overview its genetic background with future therapeutic approaches.
Keywords: Bietti crystalline dystrophy; chorioretinal dystrophy; corneal crystals; inherited disorder; vision loss.
© 2023 Saatci et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures


References
-
- Bietti G. On the familial occurrence of “retinitis punctata albescens” (associated with “dystrophia marginalis cristallinea cornea)”, glistening, vitreous humor and other degenerative ocular changes. Augenvera¨Nderungen Klin Monatsbl Augenheilkd. 1937;99:737–756.
Publication types
LinkOut - more resources
Full Text Sources
