

Sustained Perturbation of Metabolism and Metabolic Subphenotypes Are Associated With Mortality and Protein Markers of the Host Response
- PMID: 36998529
- PMCID: PMC10047616
- DOI: 10.1097/CCE.0000000000000881
Sustained Perturbation of Metabolism and Metabolic Subphenotypes Are Associated With Mortality and Protein Markers of the Host Response
Abstract
Perturbed host metabolism is increasingly recognized as a pillar of sepsis pathogenesis, yet the dynamic alterations in metabolism and its relationship to other components of the host response remain incompletely understood. We sought to identify the early host-metabolic response in patients with septic shock and to explore biophysiological phenotyping and differences in clinical outcomes among metabolic subgroups.
Design: We measured serum metabolites and proteins reflective of the host-immune and endothelial response in patients with septic shock.
Setting: We considered patients from the placebo arm of a completed phase II, randomized controlled trial conducted at 16 U.S. medical centers. Serum was collected at baseline (within 24 hr of the identification of septic shock), 24-hour, and 48-hour postenrollment. Linear mixed models were built to assess the early trajectory of protein analytes and metabolites stratified by 28-day mortality status. Unsupervised clustering of baseline metabolomics data was conducted to identify subgroups of patients.
Patients: Patients with vasopressor-dependent septic shock and moderate organ dysfunction that were enrolled in the placebo arm of a clinical trial.
Interventions: None.
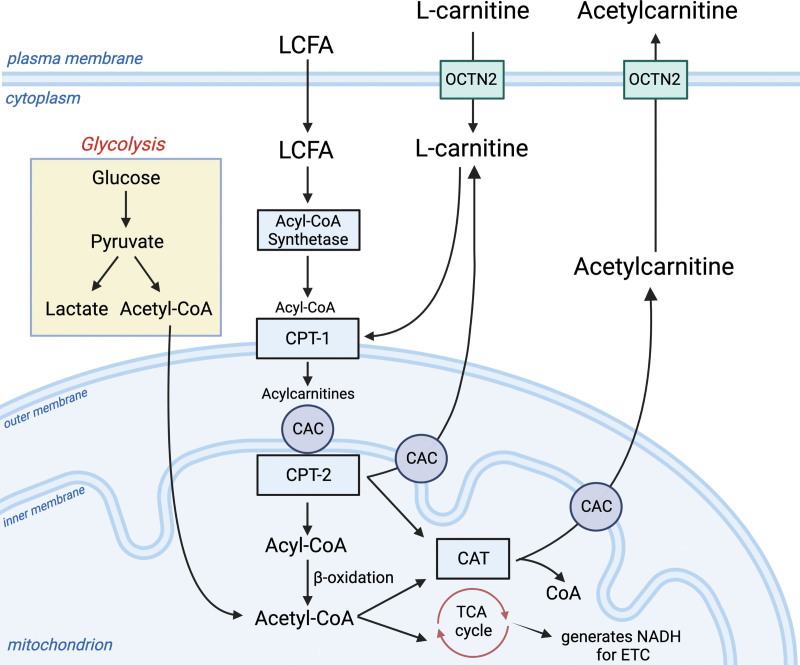
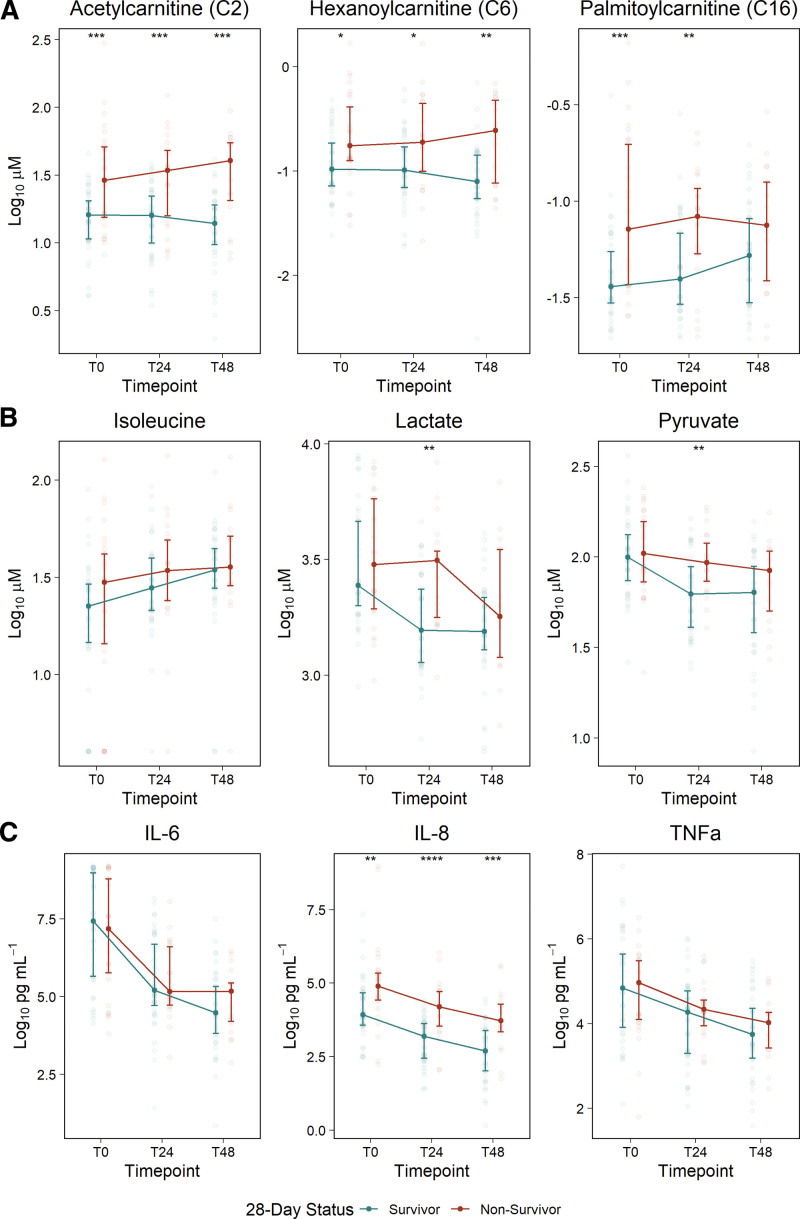
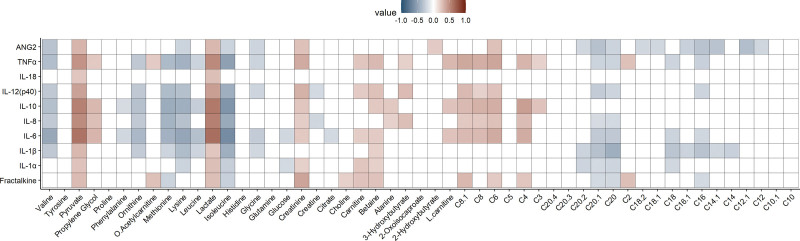
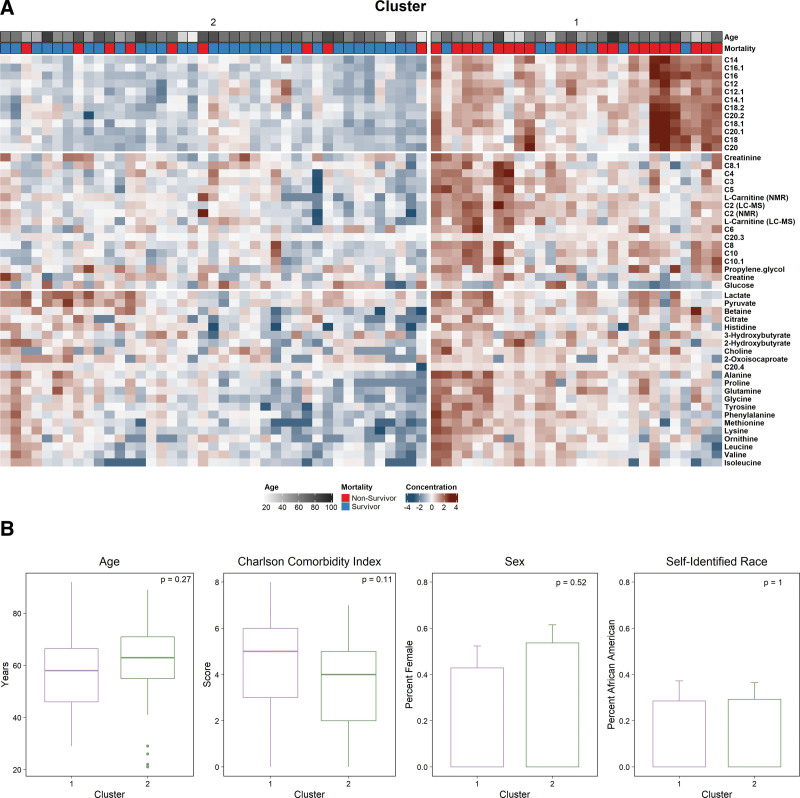
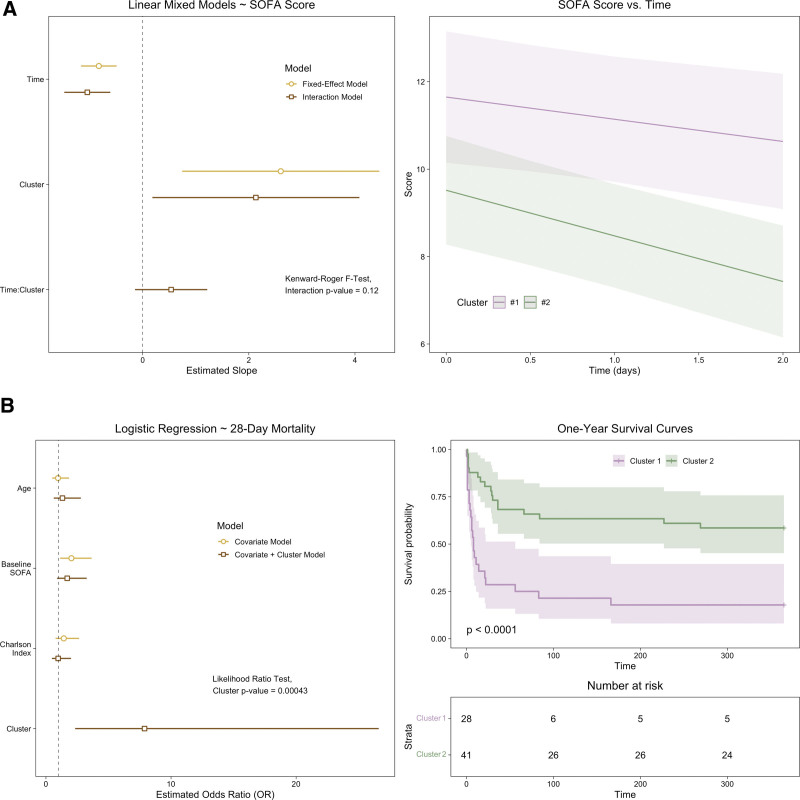
Measurements and main results: Fifty-one metabolites and 10 protein analytes were measured longitudinally in 72 patients with septic shock. In the 30 patients (41.7%) who died prior to 28 days, systemic concentrations of acylcarnitines and interleukin (IL)-8 were elevated at baseline and persisted at T24 and T48 throughout early resuscitation. Concentrations of pyruvate, IL-6, tumor necrosis factor-α, and angiopoietin-2 decreased at a slower rate in patients who died. Two groups emerged from clustering of baseline metabolites. Group 1 was characterized by higher levels of acylcarnitines, greater organ dysfunction at baseline and postresuscitation (p < 0.05), and greater mortality over 1 year (p < 0.001).
Conclusions: Among patients with septic shock, nonsurvivors exhibited a more profound and persistent dysregulation in protein analytes attributable to neutrophil activation and disruption of mitochondrial-related metabolism than survivors.
Keywords: biomarkers; chemokines; cytokines; metabolomics; precision medicine.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Jennaro is supported by the American Foundation of Pharmaceutical Education. The remaining authors have disclosed that they do not have any potential conflicts of interest. The content is solely the responsibility of the authors and does not necessarily represent the official views of National Institute of General Medical Sciences or the National Institutes of Health.
Figures
References
-
- Maslove DM, Tang B, Shankar-Hari M, et al. : Redefining critical illness. Nat Med 2022; 28:1141–1148 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
