

Preparing for the Artificial Intelligence Revolution in Nuclear Cardiology
- PMID: 36998588
- PMCID: PMC10043081
- DOI: 10.1007/s13139-021-00733-3
Preparing for the Artificial Intelligence Revolution in Nuclear Cardiology
Abstract
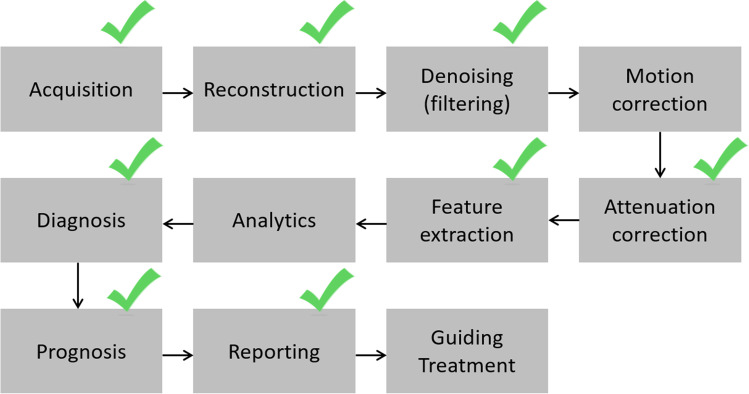
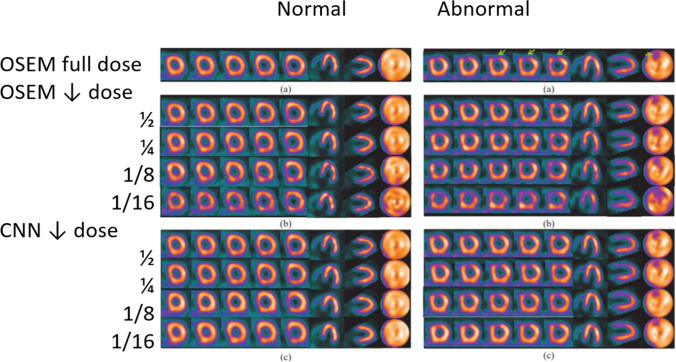
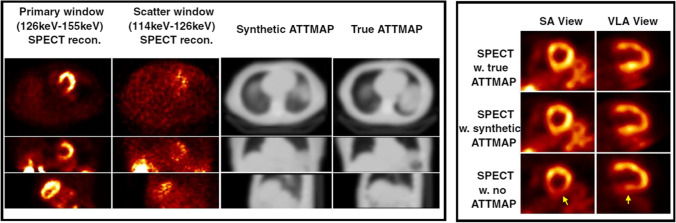
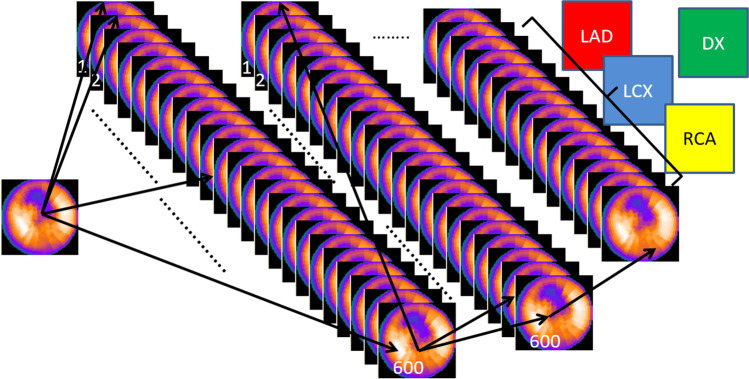
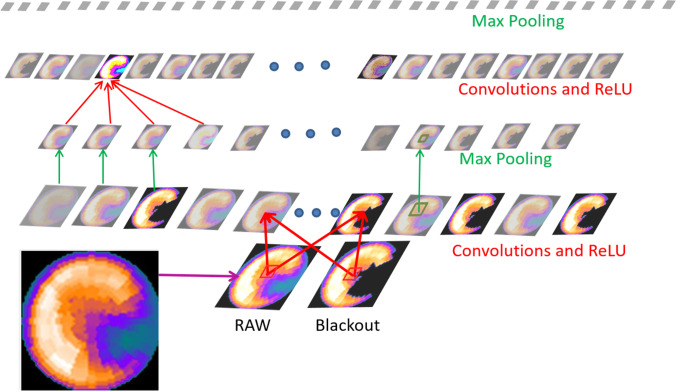
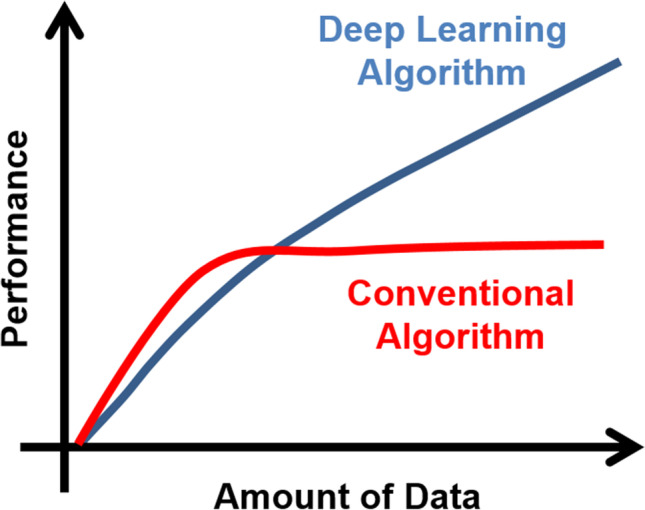
A major opportunity in nuclear cardiology is the many significant artificial intelligence (AI) applications that have recently been reported. These developments include using deep learning (DL) for reducing the needed injected dose and acquisition time in perfusion acquisitions also due to DL improvements in image reconstruction and filtering, SPECT attenuation correction using DL without need for transmission images, DL and machine learning (ML) use for feature extraction to define myocardial left ventricular (LV) borders for functional measurements and improved detection of the LV valve plane and AI, ML, and DL implementations for MPI diagnosis, prognosis, and structured reporting. Although some have, most of these applications have yet to make it to widespread commercial distribution due to the recency of their developments, most reported in 2020. We must be prepared both technically and socio-economically to fully benefit from these and a tsunami of other AI applications that are coming.
Keywords: Absolute myocardial blood flow; Artificial intelligence; Deep learning; Machine learning; Myocardial flow reserve; Nuclear cardiology.
© The Author(s), under exclusive licence to Korean Society of Nuclear Medicine 2022.
Conflict of interest statement
Conflict of InterestDr. Ernest Garcia receives royalties from the sale of the Emory Cardiac Toolbox and has equity positions with Syntermed, Inc. The terms of these arrangements have been reviewed and approved by Emory University in accordance with its conflict of interest policies. Marina Piccinelli reports no conflict of interest.
Figures
References
-
- Einstein AJ, Pascual TNB, Mercuri M, Karthikeyan G, Vitola JV, Mahmarian JJ, et al. Current worldwide nuclear cardiology practices and radiation exposure: results from the 65 country IAEA Nuclear Cardiology Protocols Cross-Sectional Study (INCAPS) Eur Heart J. 2015;36:1689–1696. doi: 10.1093/eurheartj/ehv117. - DOI - PMC - PubMed
-
- Nuclear Medicine Market Outlook Report 2018. Accessed on 12/30/2020. Available from: https://imvinfo.com/product/nuclear-medicine-market-outlook-report-2018/
Publication types
LinkOut - more resources
Full Text Sources