

Unstimulated Gluteus Maximus Sphincteroplasty for Bowel Incontinence
- PMID: 36998924
- PMCID: PMC10049812
- DOI: 10.1055/s-0042-1759499
Unstimulated Gluteus Maximus Sphincteroplasty for Bowel Incontinence
Abstract
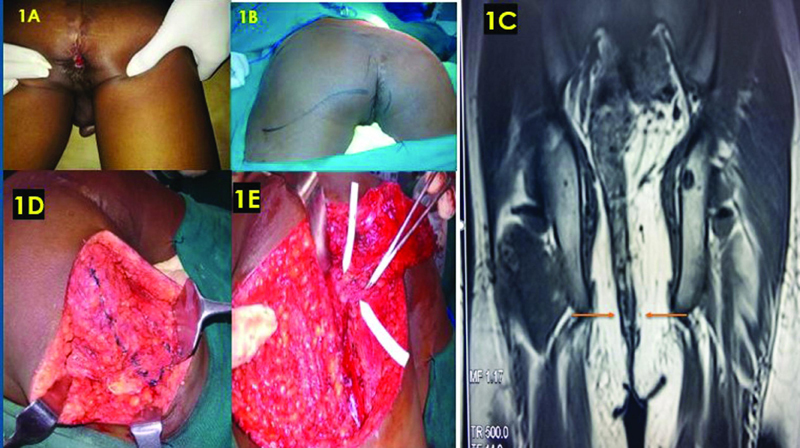
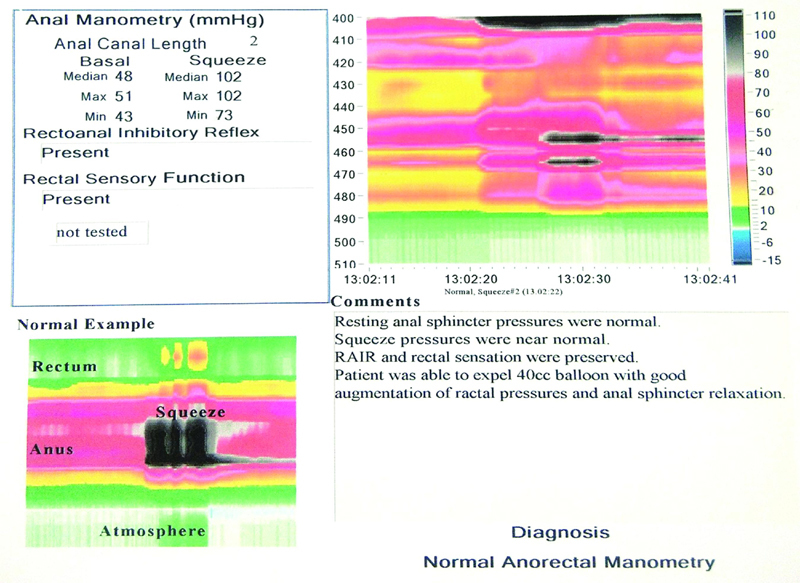
Background Gluteus maximus, by virtue of its continued adjunct contraction with the anal sphincter, has many characteristics and histomorphological features mimicking type I musculature. Hence, anal sphincter replacement therapy with gluteus maximus has all avenues for lasting successful results. This study aimed to evaluate the efficiency of unstimulated gluteus maximus sphincteroplasty for anal incontinence reconstruction and neosphincter reconstruction in perineal colostomy cases. Methods From March 2015 to March 2020, the records of patients who underwent gluteus maximus sphincteroplasty for fecal incontinence were analyzed in this retrospective cohort study. The mean age was 31.55 years. Eleven patients (females = 4, males = 7) underwent anal incontinence reconstruction. All these cases were followed up for an average period of 28.46 months. Results Good continence was observed in all patients with an average Cleveland Clinic Florida Faecal Incontinence Score of 3.18 ( p = 0.0035). At the end of the follow-up period, the average median resting pressure found via manometry was 44.64 mm Hg, and the average median squeeze pressure was 103.55mm Hg. The mean of the average continence contraction time at the end of the follow-up period was found to be 3.64 minutes. None of our patients had complete continence failure. None of our patients used perineal pads or made any lifestyle alterations at the end of the follow-up period. Most of the patients expressed satisfactory continence. Conclusion Despite being untrained with implantable electrodes, the gluteus maximus muscle produced very good continence results with our way of construct. In addition, with its good lumen occluding effect, it achieves good resting and squeeze anal pressure around the anal canal/bowel with trivial reeducation. Hence, it has become our institution's procedure of choice for anal sphincter reconstruction.
Keywords: anal incontinence; gluteus maximus sphincteroplasty; sphincteroplasty.
Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None.
Figures










References
-
- Merchea A, Larson D W. 20th ed. Canada: Elsevier; 2016. Anus; pp. 1395–1395.
-
- Whitehead W E, Wald A, Norton N J.Treatment options for fecal incontinence Dis Colon Rectum 20014401131–142., discussion 142–144 - PubMed
-
- Madoff R D, Rosen H R, Baeten C G. Safety and efficacy of dynamic muscle plasty for anal incontinence: lessons from a prospective, multicenter trial. Gastroenterology. 1999;116(03):549–556. - PubMed
-
- Standring S.Ed.Gray's Anatomy: The Anatomical Basis of Clinical Practice 40th editionSpain: Churchill Livingstone; 2008
-
- Taylor G I, Gianoutsos M P, Morris S F. The neurovascular territories of the skin and muscles: anatomic study and clinical implications. Plast Reconstr Surg. 1994;94(01):1–36. - PubMed
LinkOut - more resources
Full Text Sources