

Are Guideline-recommended Risk Classification Schemes in Pulmonary Hypertension Adequately Robust to Guide the Real-world Setting?
- PMID: 37000114
- PMCID: PMC10175884
- DOI: 10.4274/balkanmedj.galenos.2023.2023-2-22
Are Guideline-recommended Risk Classification Schemes in Pulmonary Hypertension Adequately Robust to Guide the Real-world Setting?
Abstract
Background: Pulmonary hypertension is a complex syndrome that encompasses a diverse group of pathophysiologies predisposed by different environmental and genetic factors. It is not clear to which extent the universal risk classification schemes can be applied to cohorts in individual pulmonary hypertension centers with differing environmental backgrounds, genetic pools, referral networks.
Aims: To explore whether the recommended risk classification schemes could reliably be used for mortality prediction in an unselected pulmonary hypertension population of a tertiary pulmonary hypertension center.
Study design: A retrospective cross-sectional study.
Methods: We retrospectively screened our hospital database for the patients with pulmonary hypertension between 2015 and 2022. The grouping of pulmonary hypertension was made as follows in accordance with current guidelines: Group 1: patients with pulmonary arterial hypertension, Group 2: patients with pulmonary hypertension associated with left heart disease, Group 3: patients with pulmonary hypertension associated with lung disease and/or hypoxia, and Group 4: patients with pulmonary hypertension associated with pulmonary artery obstructions. Then, we compared the predicted and observed mortality rates of four different risk classification schemes (REVEAL, REVEAL-Lite, ESC/ERS and COMPERA).
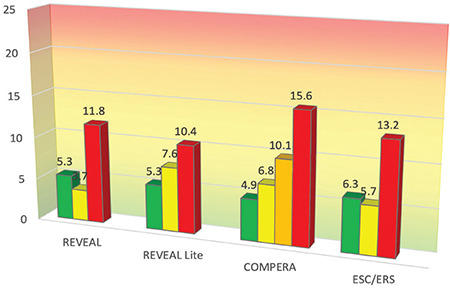
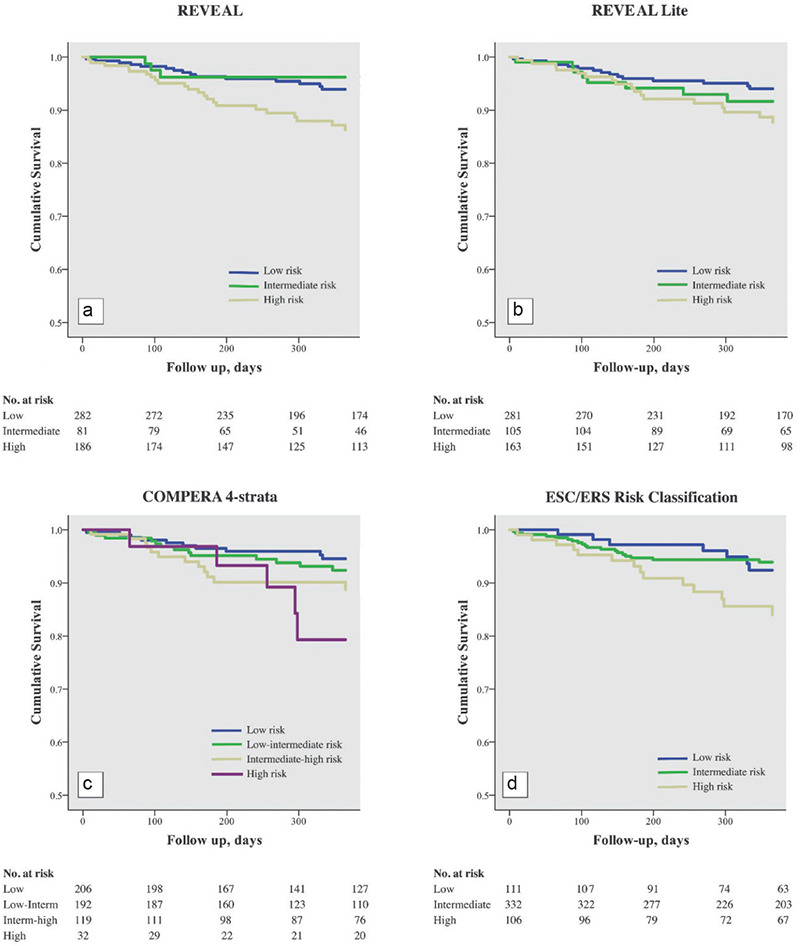
Results: We identified 723 cases in our pulmonary hypertension database, the final study population consisted of 549 patients. The REVEAL, REVEAL-Lite and European Society of Cardiology/European Respiratory Society risk scores significantly underestimated the mortality risk in the low-risk stratum (5.3% vs. 1.9%, P < 0.001; 5.3% vs. 2.9%, P = 0.015 and 6.3% vs. 1%, P < 0.001, respectively) and overestimated the mortality risk in the high-risk stratum (11.8% vs. 25.8%, P < 0.001; 10.4% vs. 25.1%, P < 0.001 and 13.2% vs. 30%, P < 0.001, respectively). Although the COMPERA 4-strata model significantly underestimated the risk in low- and intermediate-low risk strata (4.9% vs. 1.5%, P < 0.001 and 6.8% vs. 2.8%, P = 0.001, respectively), it was accurate in intermediate-high and high-risk groups (10.1% vs. 8.7%, P = 0.592 and 15.6% vs. 22%, P = 0.384, respectively). The analyses limited only to group 1 pulmonary hypertension patients gave similar results.
Conclusion: The established risk classification schemes may not perform as good as expected in unselected pulmonary hypertension populations and this may have important implications on management decisions. Tertiary centers should not uncritically accept the published risk prediction models and consider modifying current risk scores according to their own patient characteristics.
Conflict of interest statement
Figures
Similar articles
-
Comparison Between REVEAL Lite 2 and COMPERA 2.0 for Risk Stratification in Pulmonary Arterial Hypertension.Chest. 2024 Aug;166(2):373-387. doi: 10.1016/j.chest.2024.02.052. Epub 2024 Mar 4. Chest. 2024. PMID: 38447640
-
Predicting Survival in Patients With Pulmonary Arterial Hypertension: The REVEAL Risk Score Calculator 2.0 and Comparison With ESC/ERS-Based Risk Assessment Strategies.Chest. 2019 Aug;156(2):323-337. doi: 10.1016/j.chest.2019.02.004. Epub 2019 Feb 14. Chest. 2019. PMID: 30772387
-
Evaluation of the European Society of Cardiology/European Respiratory Society derived three- and four-strata risk stratification models in pulmonary arterial hypertension: introducing an internet-based risk stratification calculator.Eur Heart J Open. 2023 Feb 21;3(2):oead012. doi: 10.1093/ehjopen/oead012. eCollection 2023 Mar. Eur Heart J Open. 2023. PMID: 36959867 Free PMC article.
-
Pulmonary arterial hypertension.Orphanet J Rare Dis. 2013 Jul 6;8:97. doi: 10.1186/1750-1172-8-97. Orphanet J Rare Dis. 2013. PMID: 23829793 Free PMC article. Review.
-
Risk assessment in pulmonary arterial hypertension.Eur Respir Rev. 2016 Dec;25(142):390-398. doi: 10.1183/16000617.0077-2016. Eur Respir Rev. 2016. PMID: 27903661 Free PMC article. Review.
References
-
- Barst RJ, McGoon M, Torbicki A, et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43(12 Suppl S):40–47. - PubMed
-
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43:3618–3731. - PubMed
-
- Benza RL, Miller DP, Foreman AJ, et al. Prognostic implications of serial risk score assessments in patients with pulmonary arterial hypertension: a Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) analysis. J Heart Lung Transplant. 2015;34:356–361. - PubMed
-
- Boucly A, Weatherald J, Savale L, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50:1700889. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical