

Association Between Daily Alcohol Intake and Risk of All-Cause Mortality: A Systematic Review and Meta-analyses
- PMID: 37000449
- PMCID: PMC10066463
- DOI: 10.1001/jamanetworkopen.2023.6185
Association Between Daily Alcohol Intake and Risk of All-Cause Mortality: A Systematic Review and Meta-analyses
Erratum in
-
Errors in Figure and Supplement.JAMA Netw Open. 2023 May 1;6(5):e2315283. doi: 10.1001/jamanetworkopen.2023.15283. JAMA Netw Open. 2023. PMID: 37159205 Free PMC article. No abstract available.
Abstract
Importance: A previous meta-analysis of the association between alcohol use and all-cause mortality found no statistically significant reductions in mortality risk at low levels of consumption compared with lifetime nondrinkers. However, the risk estimates may have been affected by the number and quality of studies then available, especially those for women and younger cohorts.
Objective: To investigate the association between alcohol use and all-cause mortality, and how sources of bias may change results.
Data sources: A systematic search of PubMed and Web of Science was performed to identify studies published between January 1980 and July 2021.
Study selection: Cohort studies were identified by systematic review to facilitate comparisons of studies with and without some degree of controls for biases affecting distinctions between abstainers and drinkers. The review identified 107 studies of alcohol use and all-cause mortality published from 1980 to July 2021.
Data extraction and synthesis: Mixed linear regression models were used to model relative risks, first pooled for all studies and then stratified by cohort median age (<56 vs ≥56 years) and sex (male vs female). Data were analyzed from September 2021 to August 2022.
Main outcomes and measures: Relative risk estimates for the association between mean daily alcohol intake and all-cause mortality.
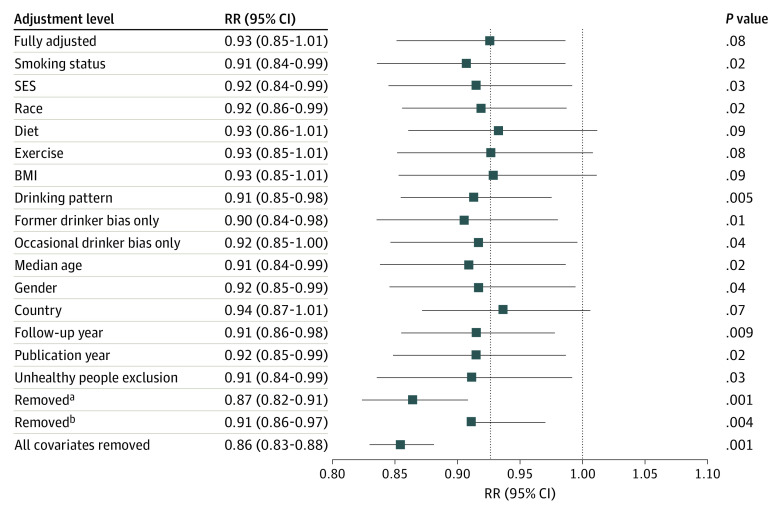
Results: There were 724 risk estimates of all-cause mortality due to alcohol intake from the 107 cohort studies (4 838 825 participants and 425 564 deaths available) for the analysis. In models adjusting for potential confounding effects of sampling variation, former drinker bias, and other prespecified study-level quality criteria, the meta-analysis of all 107 included studies found no significantly reduced risk of all-cause mortality among occasional (>0 to <1.3 g of ethanol per day; relative risk [RR], 0.96; 95% CI, 0.86-1.06; P = .41) or low-volume drinkers (1.3-24.0 g per day; RR, 0.93; P = .07) compared with lifetime nondrinkers. In the fully adjusted model, there was a nonsignificantly increased risk of all-cause mortality among drinkers who drank 25 to 44 g per day (RR, 1.05; P = .28) and significantly increased risk for drinkers who drank 45 to 64 and 65 or more grams per day (RR, 1.19 and 1.35; P < .001). There were significantly larger risks of mortality among female drinkers compared with female lifetime nondrinkers (RR, 1.22; P = .03).
Conclusions and relevance: In this updated systematic review and meta-analysis, daily low or moderate alcohol intake was not significantly associated with all-cause mortality risk, while increased risk was evident at higher consumption levels, starting at lower levels for women than men.
Conflict of interest statement
Figures
Comment in
-
ISFAR Reiterates Its Defense of Moderate Alcohol Consumption's Health Benefits.J Stud Alcohol Drugs. 2024 Jan;85(1):136-140. doi: 10.15288/jsad.23-00293. Epub 2023 Dec 11. J Stud Alcohol Drugs. 2024. PMID: 38095176 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
