

Safety and Efficacy of Ceftolozane/Tazobactam Plus Metronidazole Versus Meropenem From a Phase 2, Randomized Clinical Trial in Pediatric Participants With Complicated Intra-abdominal Infection
- PMID: 37000942
- PMCID: PMC10259210
- DOI: 10.1097/INF.0000000000003911
Safety and Efficacy of Ceftolozane/Tazobactam Plus Metronidazole Versus Meropenem From a Phase 2, Randomized Clinical Trial in Pediatric Participants With Complicated Intra-abdominal Infection
Abstract
Background: Ceftolozane/tazobactam, a cephalosporin-β-lactamase inhibitor combination, is approved for the treatment of complicated urinary tract infections and complicated intra-abdominal infections (cIAI). The safety and efficacy of ceftolozane/tazobactam in pediatric participants with cIAI were assessed.
Methods: This phase 2 study (NCT03217136) randomized participants to either ceftolozane/tazobactam+metronidazole or meropenem for treatment of cIAI in pediatric participants (<18 years). The primary objective was to assess the safety and tolerability of intravenous ceftolozane/tazobactam+metronidazole. Clinical cure at end of treatment (EOT) and test of cure (TOC) visits were secondary end points.
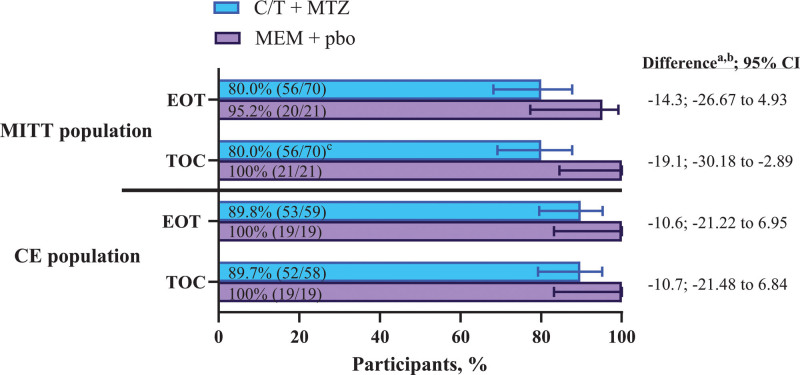
Results: The modified intent-to-treat (MITT) population included 91 participants (ceftolozane/tazobactam+metronidazole, n = 70; meropenem, n = 21). Complicated appendicitis was the most common diagnosis (93.4%); Escherichia coli was the most common pathogen (65.9%). Adverse events (AEs) occurred in 80.0% and 61.9% of participants receiving ceftolozane/tazobactam+metronidazole and meropenem, drug-related AEs occurred in 18.6% and 14.3% and serious AEs occurred in 11.4% and 0% of participants receiving ceftolozane/tazobactam+metronidazole and meropenem, respectively. No drug-related serious AEs or discontinuations due to drug-related AEs occurred. Rates of the clinical cure for ceftolozane/tazobactam+metronidazole and meropenem at EOT were 80.0% and 95.2% (difference: -14.3; 95% confidence interval: -26.67 to 4.93) and at TOC were 80.0% and 100.0% (difference: -19.1; 95% confidence interval: -30.18 to -2.89), respectively; 6 of the 14 clinical failures for ceftolozane/tazobactam+metronidazole at TOC were indeterminate responses imputed as failures per protocol.
Conclusion: Ceftolozane/tazobactam+metronidazole was well tolerated in pediatric participants with cIAI and had a safety profile similar to the established safety profile in adults. In this descriptive efficacy analysis, ceftolozane/tazobactam+metronidazole appeared efficacious.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
J.L., F.-H.S, J.A.H., M.B., M.G.J., C.D.A., E.G.R., and C.J.B. are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (MSD), who may own stock and/or hold stock options in Merck & Co., Inc., Rahway, NJ, USA. M.W.P. was an employee of MSD at the time of the study conduct. C.-C.A.J. received consulting fees from MSD and holds stock in Merck & Co., Inc., Rahway, NJ, USA. J.N. reports funding to conduct the study from MSD to his institution. N.D. has no potential conflicts of interest to disclose.
Figures
References
-
- Menichetti F, Sganga G. Definition and classification of intra-abdominal infections. J Chemother. 2009;21(suppl 1):3–4. - PubMed
-
- Newman N, Wattad E, Greenberg D, et al. . Community-acquired complicated intra-abdominal infections in children hospitalized during 1995-2004 at a paediatric surgery department. Scand J Infect Dis. 2009;41:720–726. - PubMed
-
- Lob SH, Badal RE, Hackel MA, et al. . Epidemiology and antimicrobial susceptibility of gram-negative pathogens causing intra-abdominal infections in pediatric patients in Europe-SMART 2011-2014. J Pediatric Infect Dis Soc. 2017;6:72–79. - PubMed
-
- Solomkin JS, Mazuski JE, Bradley JS, et al. . Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:133–164. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
