

QT interval and short-term outcome in acute heart failure
- PMID: 37004527
- PMCID: PMC10698082
- DOI: 10.1007/s00392-023-02173-9
QT interval and short-term outcome in acute heart failure
Abstract
Objective: To investigate the association of corrected QT (QTc) interval duration and short-term outcomes in patients with acute heart failure (AHF).
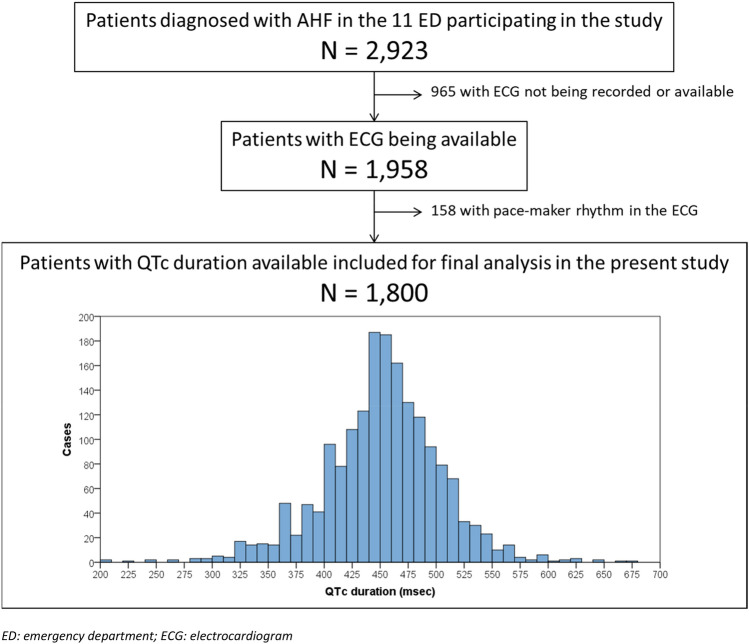
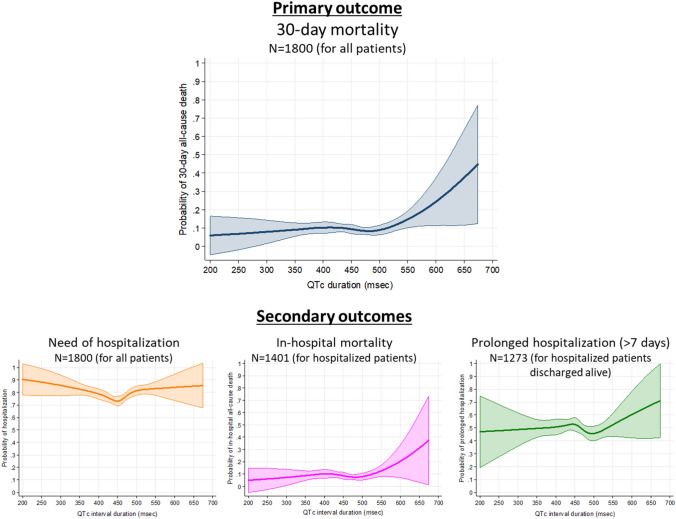
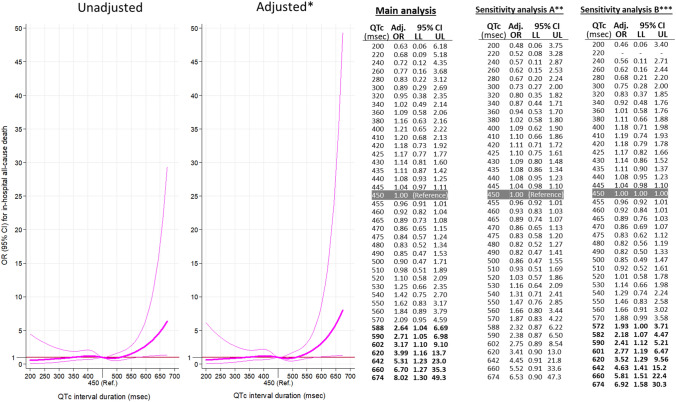
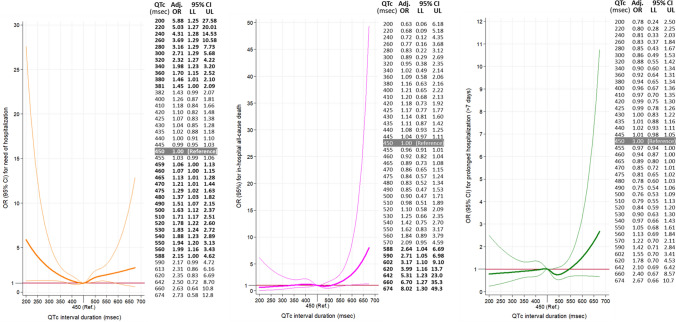
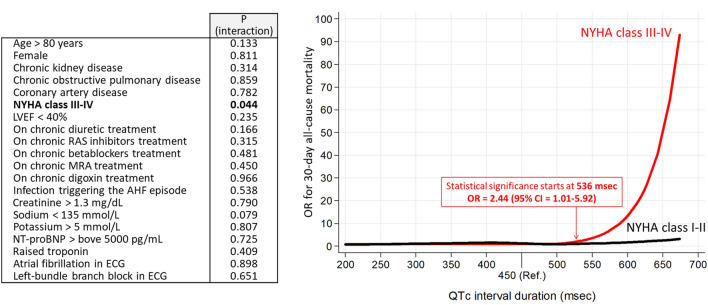
Methods: We analyzed AHF patients enrolled in 11 Spanish emergency departments (ED) for whom an ECG with QTc measurement was available. Patients with pace-maker rhythm were excluded. Primary outcome was 30-day all-cause mortality and secondary outcomes were need of hospitalization, in-hospital mortality and prolonged hospitalization (> 7 days). Association between QTc and outcomes was explored by restricted cubic spline (RCS) curves. Results were expressed as odds ratios (OR) and 95%CI adjusted by patients baseline and decompensation characteristics, using a QTc = 450 ms as reference.
Results: Of 1800 patients meeting entry criteria (median age 84 years (IQR = 77-89), 56% female), their median QTc was 453 ms (IQR = 422-483). The 30-day mortality was 9.7%, while need of hospitalization, in-hospital mortality and prolonged hospitalization were 77.8%, 9.0% and 50.0%, respectively. RCS curves found longer QTc was associated with 30-day mortality if > 561 ms, OR = 1.86 (1.00-3.45), and increased up to OR = 10.5 (2.25-49.1), for QTc = 674 ms. A similar pattern was observed for in-hospital mortality; OR = 2.64 (1.04-6.69), for QTc = 588 ms, and increasing up to OR = 8.02 (1.30-49.3), for QTc = 674 ms. Conversely, the need of hospitalization had a U-shaped relationship: being increased in patients with shorter QTc [OR = 1.45 (1.00-2.09) for QTc = 381 ms, OR = 5.88 (1.25-27.6) for the shortest QTc of 200 ms], and also increasing for prolonged QTc [OR = 1.06 (1.00-1.13), for QTc = 459 ms, and reaching OR = 2.15 (1.00-4.62) for QTc = 588 ms]. QTc was not associated with prolonged hospitalization.
Conclusion: In ED AHF patients, initial QTc provides independent short-term prognostic information, with increasing QTc associated with increasing mortality, while both, shortened and prolonged QTc are associated with need of hospitalization.
Keywords: Acute heart failure; Electrocardiogram; Emergency department; Mortality; Outcome; QTc interval.
© 2023. The Author(s).
Conflict of interest statement
The authors state that they have no conflict of interests with the present work. The ICA-SEMES Research Group has received unrestricted support from Orion Pharma, Novartis and Boehringer. The present study has been designed, performed, analyzed and written exclusively by the authors independently of these pharmaceutical companies.
Figures
References
-
- Miró Ò, García Sarasola A, Fuenzalida C, Calderón S, Jacob J, Aguirre A, et al. Departments involved during the first episode of acute heart failure and subsequent emergency department revisits and rehospitalisations: an outlook through the NOVICA cohort. Eur J Heart Fail. 2019;21:1231–1244. doi: 10.1002/ejhf.1567. - DOI - PubMed
-
- García-Álvarez A. Safety and the identification of modifiable factors in older patients discharged from the emergency department with acute heart failure. Emergencias. 2021;33(3):161–162. - PubMed
