

AXL Expression on Homeostatic Resident Liver Macrophages Is Reduced in Cirrhosis Following GAS6 Production by Hepatic Stellate Cells
- PMID: 37004869
- PMCID: PMC10209017
- DOI: 10.1016/j.jcmgh.2023.03.007
AXL Expression on Homeostatic Resident Liver Macrophages Is Reduced in Cirrhosis Following GAS6 Production by Hepatic Stellate Cells
Abstract
Background & aims: AXL and MERTK expression on circulating monocytes modulated immune responses in patients with cirrhosis (CD14+HLA-DR+AXL+) and acute-on-chronic liver failure (CD14+MERTK+). AXL expression involved enhanced efferocytosis, sustained phagocytosis, but reduced tumor necrosis factor-α/interleukin-6 production and T-cell activation, suggesting a homeostatic function. Axl was expressed on murine airway in tissues contacting the external environment, but not interstitial lung- and tissue-resident synovial lining macrophages. Here, we assessed AXL expression on tissue macrophages in patients with cirrhosis.
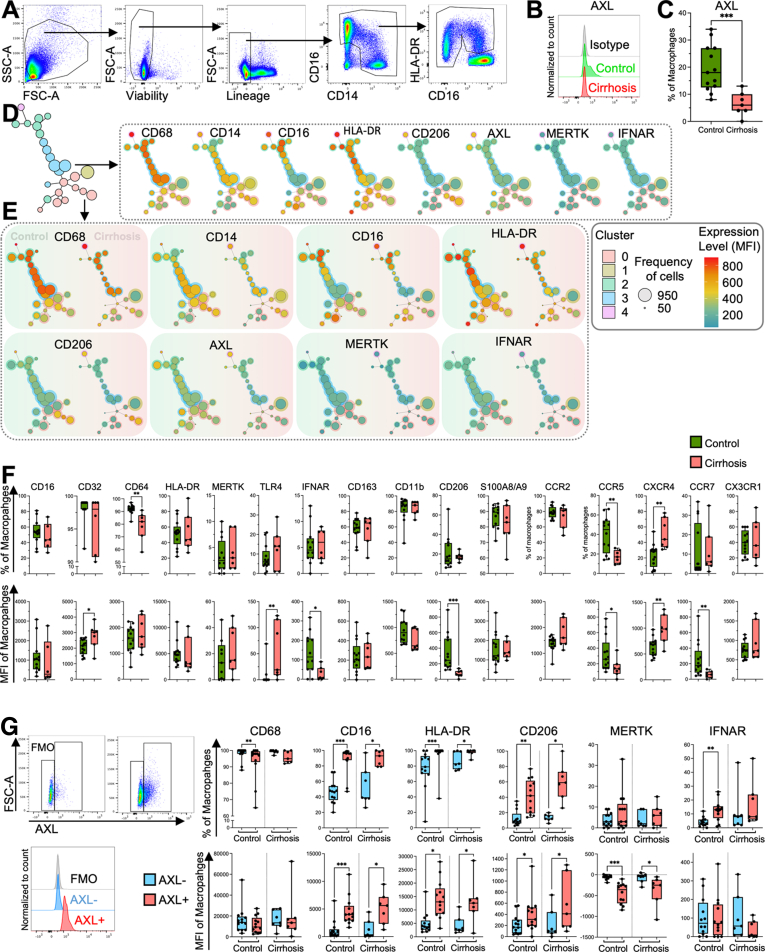
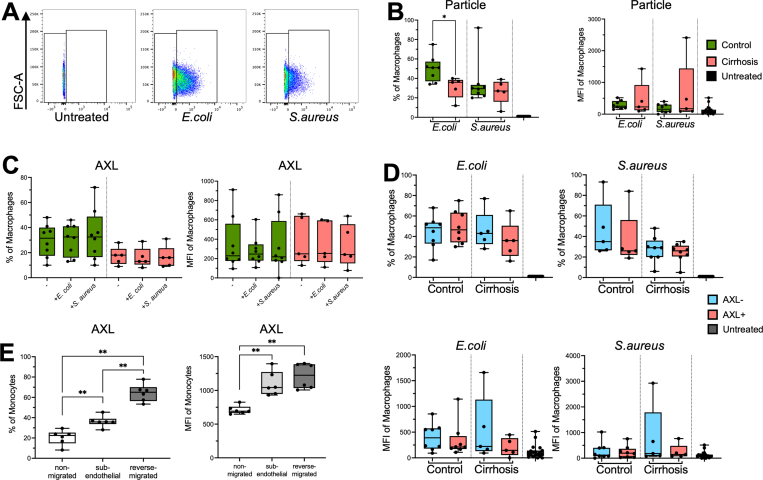
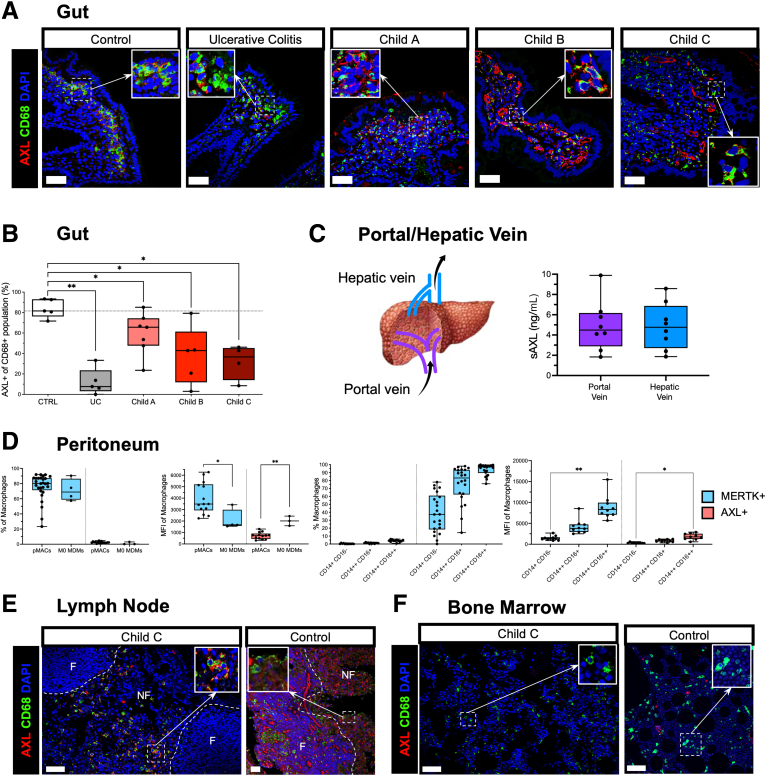
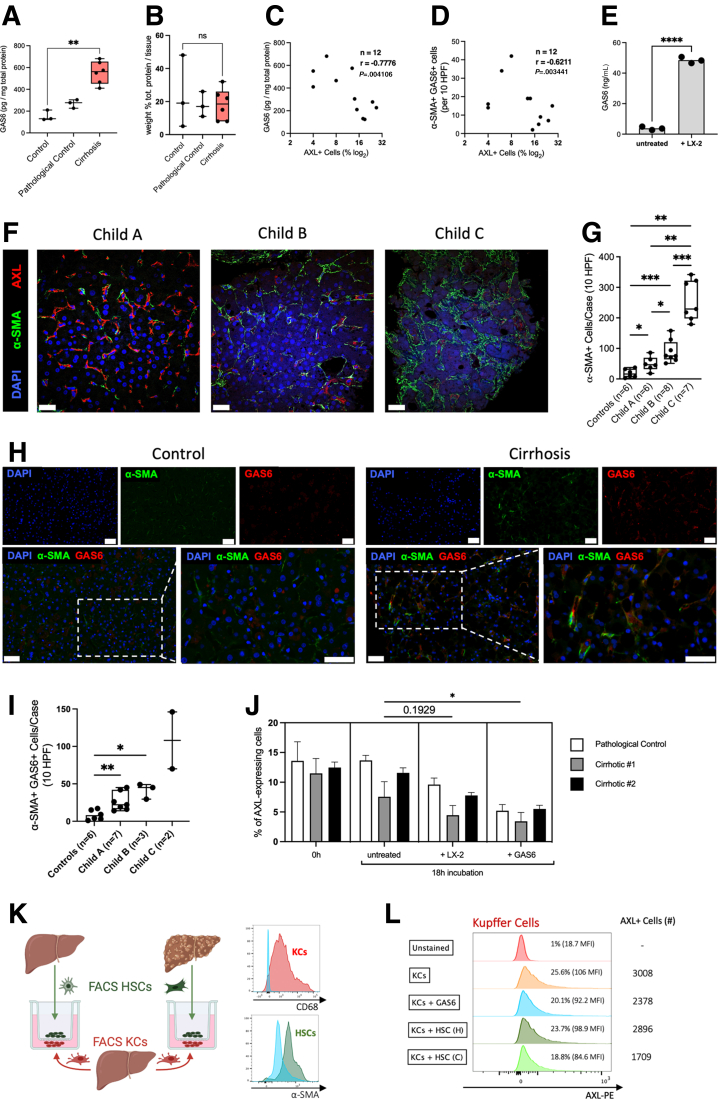
Methods: Using multiplexed immunofluorescence we compared AXL expression in liver biopsies in cirrhosis (n = 22), chronic liver disease (n = 8), non-cirrhotic portal hypertension (n = 4), and healthy controls (n = 4). Phenotype and function of isolated primary human liver macrophages were characterized by flow cytometry (cirrhosis, n = 11; control, n = 14) ex vivo. Also, AXL expression was assessed on peritoneal (n = 29) and gut macrophages (n = 16) from cirrhotic patients. Regulation of AXL expression was analyzed in vitro and ex vivo using primary hepatic stellate cells (HSCs), LX-2 cells, and GAS6 in co-culture experiments.
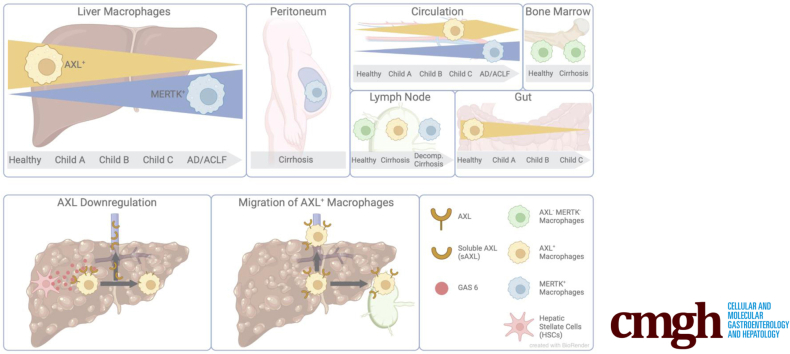
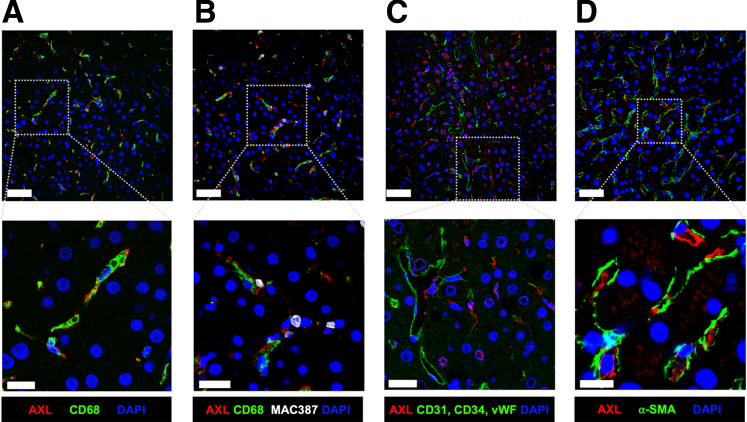
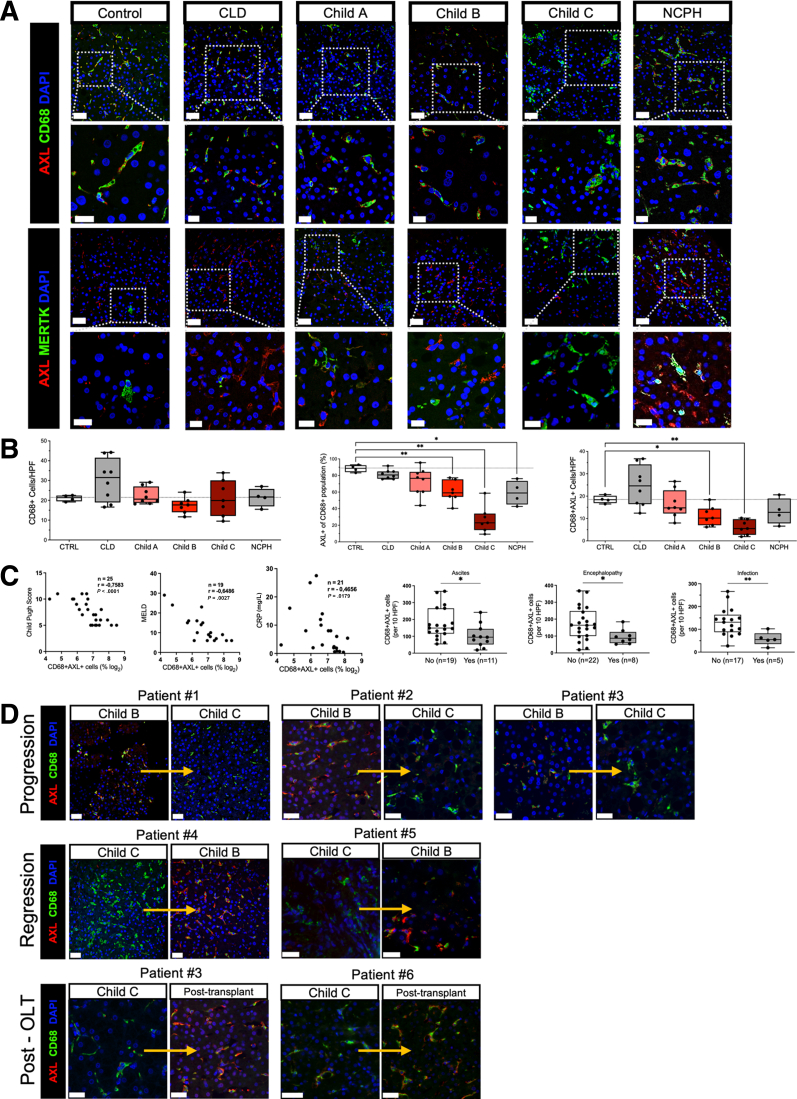
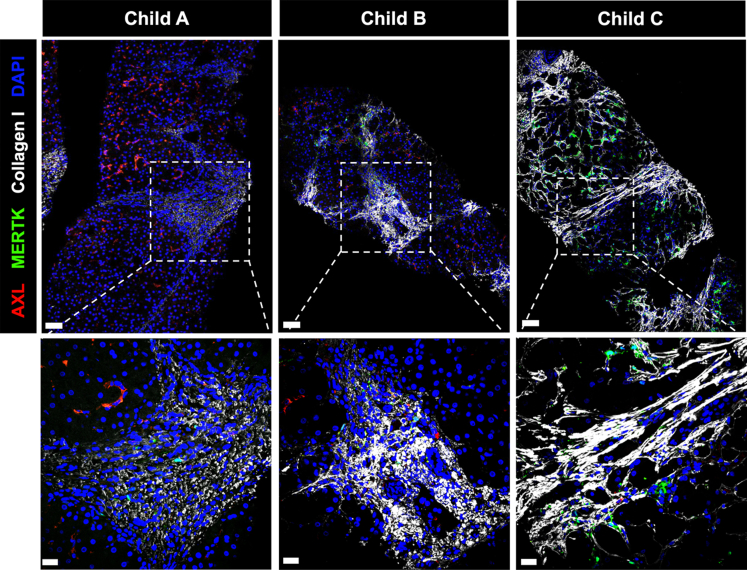
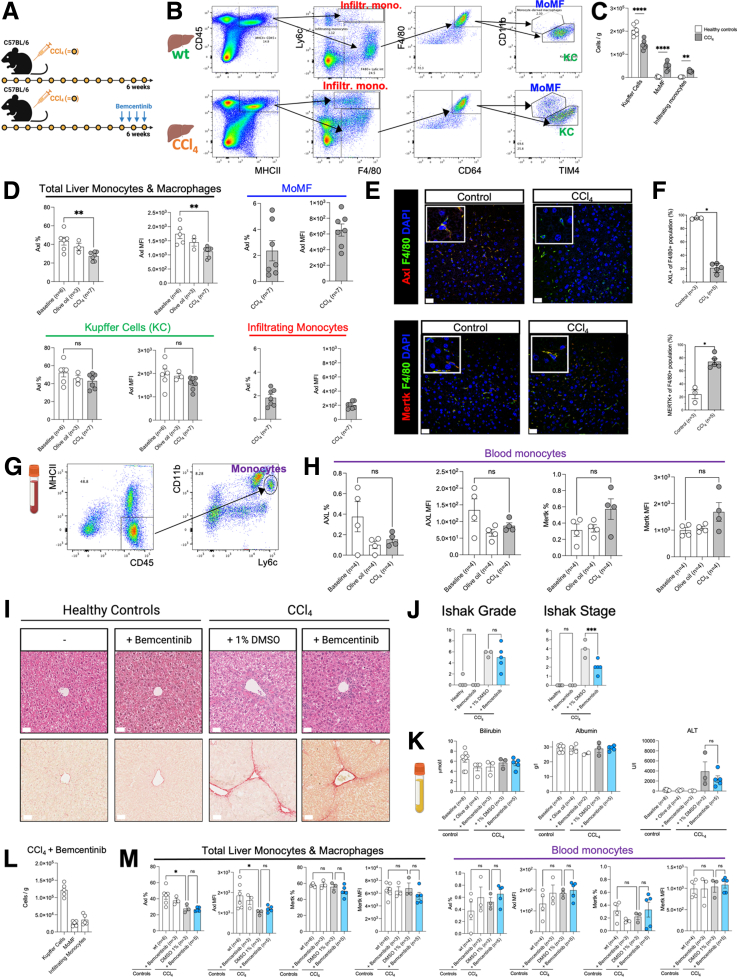
Results: AXL was expressed on resident (CD68+) but not tissue-infiltrating (MAC387+) liver macrophages, hepatocytes, HSCs, or sinusoidal endothelial cells. Prevalence of hepatic CD68+AXL+ cells significantly decreased with cirrhosis progression: (healthy, 90.2%; Child-Pugh A, 76.1%; Child-Pugh B, 64.5%; and Child-Pugh C, 18.7%; all P < .05) and negatively correlated with Model for End-Stage Liver Disease and C-reactive protein (all P < .05). AXL-expressing hepatic macrophages were CD68highHLA-DRhighCD16highCD206high. AXL expression also decreased on gut and peritoneal macrophages from cirrhotic patients but increased in regional lymph nodes. GAS6, enriched in the cirrhotic liver, appeared to be secreted by HSCs and down-regulate AXL in vitro.
Conclusions: Decreased AXL expression on resident liver macrophages in advanced cirrhosis, potentially in response to activated HSC-secreted GAS6, suggests a role for AXL in the regulation of hepatic immune homeostasis.
Keywords: Cirrhosis; Innate Immunity; Resident Liver Macrophages; TAM Receptors.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Balmer M.L., Slack E., Gottardi A de, et al. The liver may act as a firewall mediating mutualism between the host and its gut commensal microbiota. Sci Transl Med. 2014;6 - PubMed
-
- Bernsmeier C., van der Merwe S., Périanin A. Innate immune cells in cirrhosis. J Hepatol. 2020;73:186–201. - PubMed
-
- Albillos A., Lario M., Álvarez-Mon M. Cirrhosis-associated immune dysfunction: distinctive features and clinical relevance. J Hepatol. 2014;61:1385–1396. - PubMed
-
- Wiest R., Lawson M., Geuking M. Pathological bacterial translocation in liver cirrhosis. J Hepatol. 2014;60:197–209. - PubMed
-
- Stengel S., Quickert S., Lutz P., et al. Peritoneal level of CD206 associates with mortality and an inflammatory macrophage phenotype in patients with decompensated cirrhosis and spontaneous bacterial peritonitis. Gastroenterology. 2020;158:1745–1761. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
