

Comparative Effectiveness of Anti-TNF in Combination With Low-Dose Methotrexate vs Anti-TNF Monotherapy in Pediatric Crohn's Disease: A Pragmatic Randomized Trial
- PMID: 37004887
- PMCID: PMC10330864
- DOI: 10.1053/j.gastro.2023.03.224
Comparative Effectiveness of Anti-TNF in Combination With Low-Dose Methotrexate vs Anti-TNF Monotherapy in Pediatric Crohn's Disease: A Pragmatic Randomized Trial
Abstract
Background & aims: Tumor necrosis factor inhibitors, including infliximab and adalimumab, are a mainstay of pediatric Crohn's disease therapy; however, nonresponse and loss of response are common. As combination therapy with methotrexate may improve response, we performed a multicenter, randomized, double-blind, placebo-controlled pragmatic trial to compare tumor necrosis factor inhibitors with oral methotrexate to tumor necrosis factor inhibitor monotherapy.
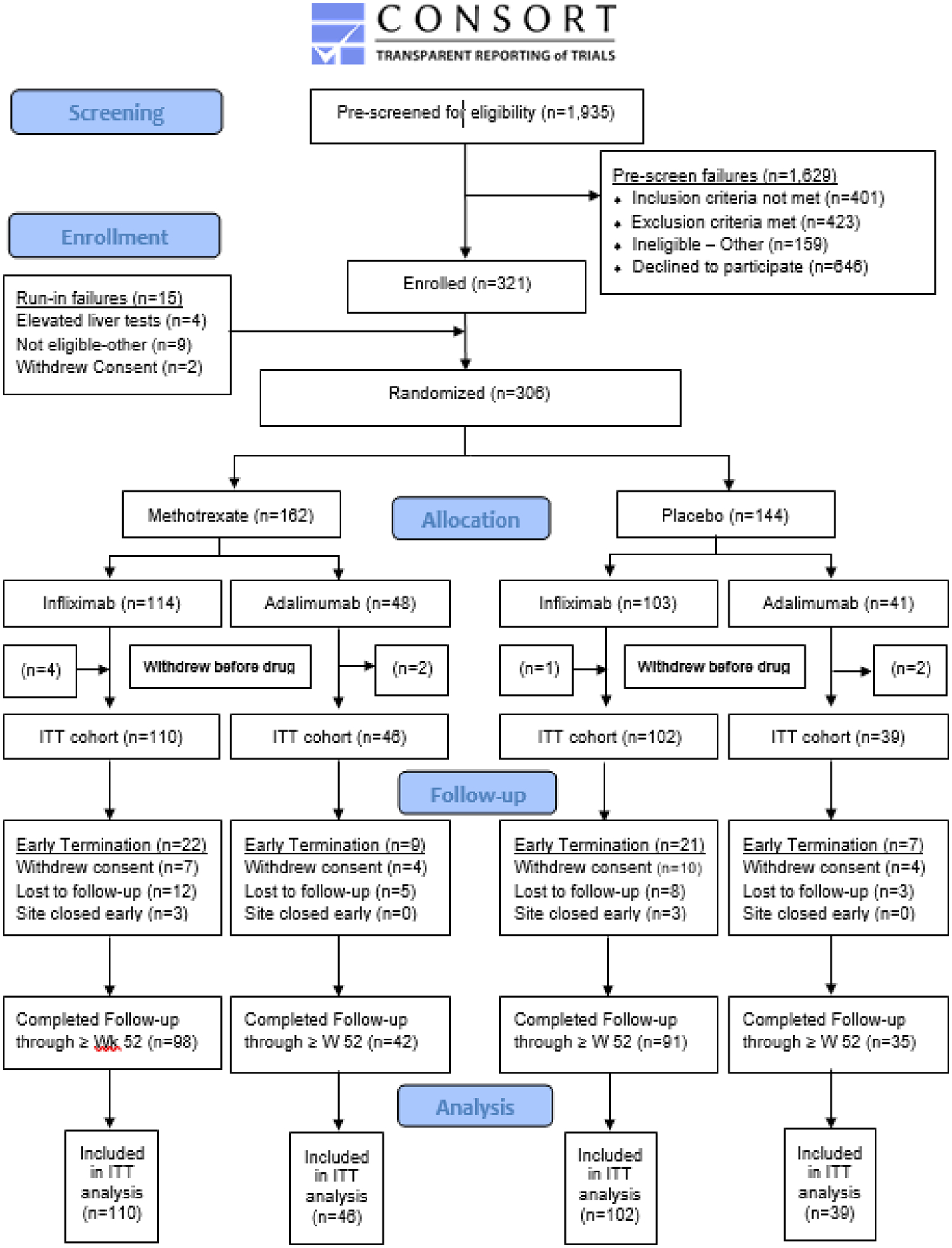
Methods: Patients with pediatric Crohn's disease initiating infliximab or adalimumab were randomized in 1:1 allocation to methotrexate or placebo and followed for 12-36 months. The primary outcome was a composite indicator of treatment failure. Secondary outcomes included anti-drug antibodies and patient-reported outcomes of pain interference and fatigue. Adverse events (AEs) and serious AEs (SAEs) were collected.
Results: Of 297 participants (mean age, 13.9 years, 35% were female), 156 were assigned to methotrexate (110 infliximab initiators and 46 adalimumab initiators) and 141 to placebo (102 infliximab initiators and 39 adalimumab initiators). In the overall population, time to treatment failure did not differ by study arm (hazard ratio, 0.69; 95% CI, 0.45-1.05). Among infliximab initiators, there were no differences between combination and monotherapy (hazard ratio, 0.93; 95% CI, 0.55-1.56). Among adalimumab initiators, combination therapy was associated with longer time to treatment failure (hazard ratio, 0.40; 95% CI, 0.19-0.81). A trend toward lower anti-drug antibody development in the combination therapy arm was not significant (infliximab: odds ratio, 0.72; 95% CI, 0.49-1.07; adalimumab: odds ratio, 0.71; 95% CI, 0.24-2.07). No differences in patient-reported outcomes were observed. Combination therapy resulted in more AEs but fewer SAEs.
Conclusions: Among adalimumab but not infliximab initiators, patients with pediatric Crohn's disease treated with methotrexate combination therapy experienced a 2-fold reduction in treatment failure with a tolerable safety profile.
Clinicaltrials: gov, Number: NCT02772965.
Keywords: Adalimumab; Anti-Tumor Necrosis Factor–α; Children; Crohn’s Disease; Infliximab; Methotrexate.
Copyright © 2023 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
MDK has consulted for Abbvie, Janssen, Pfizer, Takeda, and Lilly, is a shareholder in Johnson & Johnson, and has received research support from Pfizer, Takeda, Janssen, Abbvie, Lilly, Genentech, Boehringer Ingelheim, Bristol Myers Squibb, Celtrion, and Arenapharm.
DAW – no disclosures
HHF has consulted for Alivio, BMS, Boehringer, ExeGi Pharma, Finch, Fresenius Kabi, Gilead, Janssen, Otsuka, Pfizer, Pure Tech, Ventyx and has received research support form Allakos, Artizan, NovoNordisk, Pfizer.
AMF – no disclosures
JA – no disclosures
RFA – no disclosures
JEA – no disclosures
DMB – no disclosures
JAB – no disclosures
KB – no disclosures
CBT – no disclosures
MEB – no disclosures
BMB – no disclosures
WBB has common stock holdings in the following publicly traded companies: Pfizer, Merck, Abbott Laboratories, Viatris, and Johnson & Johnson.
JMC – no disclosures
KC – no disclosures
RBC has consulted for Janssen Research & Development and is a member of the scientific advisory board for Janssen Biotech.
CMD – no disclosures
JMD – no disclosures
DRE – no disclosures
EE - no disclosures
CBF – no disclosures
JAG – no disclosures
JEG – no disclosures
ASG – no disclosures
AI – no disclosures
TWJ has received research support from Abbvie.
JLK – no disclosures
SK – no disclosures
MEK – no disclosures
IHL – no disclosures
TML – no disclosures
EAL has received research support from Pfizer, Inc.
PAM – no disclosures
PM – no disclosures
ZMR – no disclosures
JM is on the Speaker’s Bureau for AbbVie and on the scientific medical advisory board for PSI Inc.
KO – no disclosures
LO - no disclosures
PJP – no disclosures
HP – no disclosures
KTP – no disclosures
DSP has received research support from Janssen and Abbvie.
LP – no disclosures
MR – no disclosures
CMS – no disclosures
KCS – no disclosures
JRS – no disclosures
MS – no disclosures
KAS – no disclosures
SJS – no disclosures
JAS – no disclosures
JSS – no disclosures
JT – no disclosures
PW – no disclosures
MZ – no disclosures
MW – no disclosures
AB has consulted for Takeda, Best Doctors, Eli Lilly, Fresenius Kabi, and has received research support from Janssen, Abbvie, Takeda, Buhlmann, Arena, Eli Lilly, Bristol Myers Squibb, PROCISE diagnostics.
Figures

Comment in
-
Combination therapy with methotrexate in paediatric Crohn's disease.Nat Rev Gastroenterol Hepatol. 2023 Jun;20(6):344. doi: 10.1038/s41575-023-00788-x. Nat Rev Gastroenterol Hepatol. 2023. PMID: 37085618 No abstract available.
References
-
- Burisch J, Jess T, Martinato M, et al. The burden of inflammatory bowel disease in Europe. Journal of Crohn’s and Colitis 2013;7:322–337. - PubMed
-
- Debruyn JC, Soon IS, Hubbard J, et al. Nationwide temporal trends in incidence of hospitalization and surgical intestinal resection in pediatric inflammatory bowel diseases in the United States from 1997 to 2009. Inflamm Bowel Dis 2013;19:2423–32. - PubMed
-
- Longobardi T, Jacobs P, Bernstein CN. Work losses related to inflammatory bowel disease in the United States: results from the National Health Interview Survey. Am J Gastroenterol 2003;98:1064–72. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
