

Can government subsidies and public mechanisms alleviate the physical and mental health vulnerability of China's urban and rural residents?
- PMID: 37005599
- PMCID: PMC10067002
- DOI: 10.1186/s12939-022-01805-2
Can government subsidies and public mechanisms alleviate the physical and mental health vulnerability of China's urban and rural residents?
Abstract
Background: Poverty vulnerability has been defined as the likelihood of a family falling into poverty in the upcoming months. Inequality is a major cause of poverty vulnerability in developing countries. There is evidence that establishing effective government subsidies and public service mechanisms significantly reduces health poverty vulnerability. One of the ways to study poverty vulnerability is by using empirical data such as income elasticity of demand to perform the analysis. Income elasticity refers to the extent to which changes in consumers' income affect changes in demand for commodities or public goods. In this work, we assess health poverty vulnerability in rural and urban China. We provide two levels of evidence on the marginal effects of the design and implementation of government subsidies and public mechanisms in reducing health poverty vulnerability, before and after incorporating the income elasticity of demand for health.
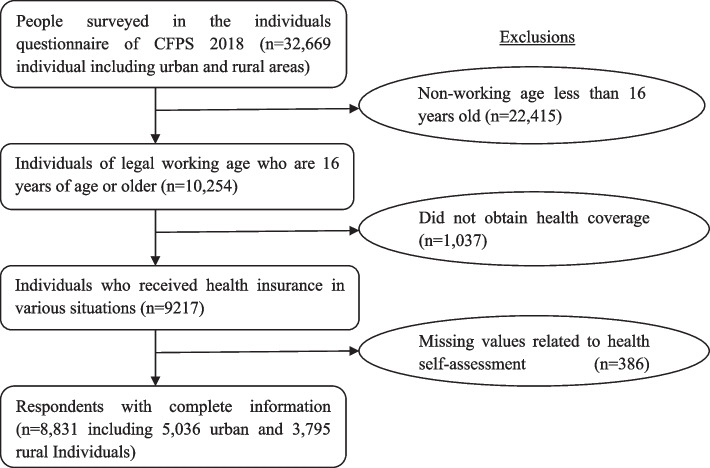
Methods: Multidimensional physical and mental health poverty indexes, according to the Oxford Poverty & Human Development Initiative and the Andersen model, were implemented to measure health poverty vulnerability by using the 2018 China Family Panel Survey database (CFPS) as the data source for empirical analysis. The income elasticity of demand for health care was used as the key mediating variable of impact. Our assessment was conducted by a two-level multidimensional logistic regression using STATA16 software.
Results: The first level regression indicates that the marginal utility of public mechanism (PM) in reducing urban and rural vulnerability as expected poverty on physical and mental health (VEP-PH&MH) was insignificant. On the other hand, government subsidies (GS) policies had a positive suppression effect on VEP-PH&MH to a relatively low degree. The second level regression found that given the diversity of health needs across individual households, i.e., the income elasticity of demand (HE) for health care products, PM and GS policies have a significant effect in reducing VEP-PH&MH in rural and urban areas. Our analysis has verified the significant positive impact of enacting accurate GS and PM policies on effectively reducing VEP-PH&MH in rural as well as urban areas.
Conclusions: This study shows that implementing government subsidies and public mechanisms has a positive marginal effect on reducing VEP-PH&MH. Meanwhile, there are individual variations in health demands, urban-rural disparities, and regional disparities in the effects of GS and PM on inhibiting VEP-PH&MH. Therefore, special consideration needs to be given to the differences in the degree of health needs of individual residents among urban and rural areas and regions with varying economic development. Furthermore, considerations of this approach in the current worldwide scenario are analyzed.
Keywords: Andersen model; Government subsidies; Multivariate logistic regression analysis; Physical and mental health poverty vulnerability index; Public mechanisms.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- WHO . Primary health care on the road to universal health coverage: 2019 global monitoring report. 2019.
-
- Pires LN, de Carvalho LB, Rawet EL. Multi-dimensional inequality and COVID-19 in Brazil. Investig Económica. 2021;80(315):33–58. doi: 10.22201/fe.01851667p.2021.315.77390. - DOI
-
- Alkire S, Roche JM, Ballon P, Foster J, Santos ME, Seth S. Multidimensional poverty measurement and analysis. New York: Oxford University Press; 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
