

Combining glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) in patients with type 2 diabetes mellitus (T2DM)
- PMID: 37005640
- PMCID: PMC10067319
- DOI: 10.1186/s12933-023-01798-4
Combining glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) in patients with type 2 diabetes mellitus (T2DM)
Abstract
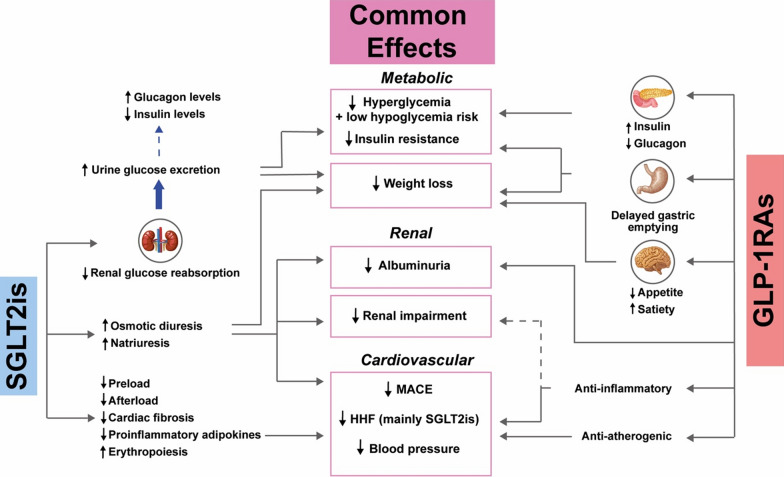
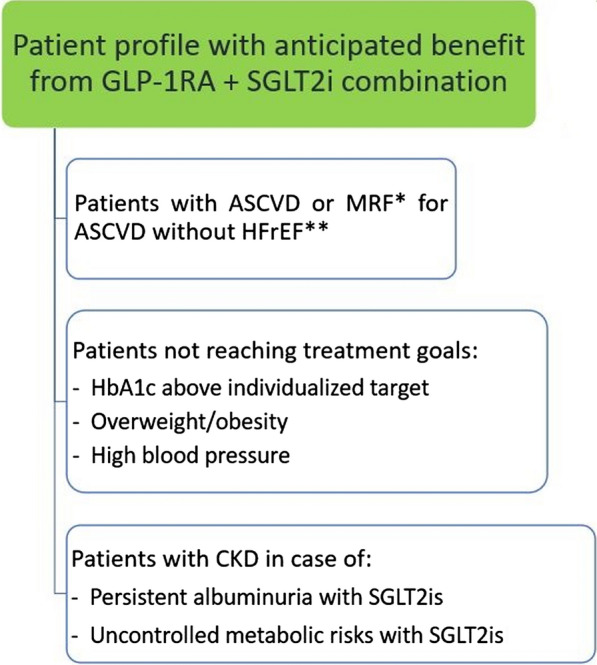
Due to their cardiovascular protective effect, glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) represent breakthrough therapies for type 2 diabetes mellitus (T2DM). In this review article, we discuss the mechanistic and clinical synergies that make the combined use of GLP-1RAs and SGLT2is appealing in patients with T2DM. Overall, the presented cumulative evidence supports the benefits of GLP-1RA plus SGLT2i combination therapy on metabolic-cardiovascular-renal disease in patients with T2DM, with a low hypoglycemia risk. Accordingly, we encourage the adoption of GLP-1RA plus SGLT2i combination therapy in patients with T2DM and established atherosclerotic cardiovascular disease (ASCVD) or multiple risk factors for ASCVD (i.e., age ≥ 55 years, overweight/obesity, dyslipidemia, hypertension, current tobacco use, left ventricular hypertrophy, and/or proteinuria). Regarding renal effects, the evidence of SGLT2is in preventing kidney failure is more abundant than for GLP-1RAs, which showed a beneficial effect on albuminuria but not on hard kidney endpoints. Hence, in case of persistent albuminuria and/or uncontrolled metabolic risks (i.e., inadequate glycemic control, hypertension, overweight/obesity) on SGLT2i therapy, GLP-1RAs should be considered as the preferential add-on therapy in T2DM patients with chronic kidney disease. Despite the potential clinical benefits of GLP-1RA plus SGLT2i combination therapy in patients with T2DM, several factors may delay this combination to become a common practice soon, such as reimbursement and costs associated with polypharmacy. Altogether, when administering GLP-1RA plus SGLT2i combination therapy, it is important to adopt an individualized approach to therapy taking into account individual preferences, costs and coverage, toxicity profile, consideration of kidney function and glucose-lowering efficacy, desire for weight loss, and comorbidities.
Keywords: Cardiovascular protection; Combination therapy; Glucagon-like peptide-1 receptor agonists; Sodium-glucose cotransporter-2 inhibitors; Type 2 diabetes mellitus.
© 2023. The Author(s).
Conflict of interest statement
PG has received occasional fees, either personally or institutionally, for the activities of speaking, scientific advising, or clinical research from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Gilead, GlaxoSmithKline, Merck Sharp & Dohme, Novo Nordisk, Organon, Pfizer, and Sanofi. PD has received consulting fees/honoraria from Novo Nordisk, Eli Lilly, Sanofi, AstraZeneca, Boehringer Ingelheim, Mundipharma, Merck Sharp & Dohme, Bayer, Abbott, LVL Medical, and Bastide. FD has received occasional consulting fees/honoraria and travel grants from BMS-Pfizer Alliance, Amgen, AstraZeneca, Bayer, Bouchara-Recordati, Bristol Myers Squibb, Boehringer Ingelheim, Menarini, Merck Sharp & Dohme, Novartis, Novo Nordisk, Organon, Pfizer, Sanofi, and Servier. JMH has received honoraria and/or travel grants from Ablynx, Alexion, AstraZeneca Rare Disease, AstraZeneca, Bayer, Bouchara-Recordati, Fresenius, GlaxoSmithKline, Mundipharma, Merck Sharp & Dohme, Roche, Servier, Sanofi, and Vifor Fresenius. BG has received fees for the activities of speaking, scientific advising, or clinical research from Eli Lilly, Novo Nordisk, AstraZeneca, Sanofi, Bristol Myers Squibb, Novartis, GlaxoSmithKline, Johnson & Johnson, Bayer, Intercept Pharma France, Gilead, Boehringer Ingelheim, Janssen, Intarcia, MetaCure, Pfizer, Merck Sharp & Dohme, Roche Diagnostics, Medtronic, Insulet, A. Menarini Diagnostics, Abbott, LifeScan, Dinno Santé, Asten Santé, Elivie, Homeperf, ISIS Diabète, Linde Homecare France, Nestlé, ORKYN’, and VitalAire.
Figures
References
-
- Díaz-Trastoy O, Villar-Taibo R, Sifontes-Dubón M, Mozo-Peñalver H, Bernabeu-Morón I, Cabezas-Agrícola JM, et al. GLP1 receptor agonist and SGLT2 inhibitor combination: an effective approach in real-world clinical practice. Clin Ther. 2020;42(2):e1–e12. doi: 10.1016/j.clinthera.2019.12.012. - DOI - PubMed
-
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Furtado RHM, et al. Comparison of the effects of glucagon-like peptide receptor agonists and sodium-glucose cotransporter 2 inhibitors for prevention of major adverse cardiovascular and renal outcomes in type 2 diabetes mellitus. Circulation. 2019;139(17):2022–2031. doi: 10.1161/CIRCULATIONAHA.118.038868. - DOI - PubMed
-
- Goldenberg RM, Ahooja V, Clemens KK, Gilbert JD, Poddar M, Verma S. Practical considerations and rationale for glucagon-like peptide-1 receptor agonist plus sodium-dependent glucose cotransporter-2 inhibitor combination therapy in type 2 diabetes. Can J Diabetes. 2021;45(3):291–302. doi: 10.1016/j.jcjd.2020.09.005. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
