

Development and validation of a glioma-associated mesenchymal stem cell-related gene prognostic index for predicting prognosis and guiding individualized therapy in glioma
- PMID: 37005685
- PMCID: PMC10068170
- DOI: 10.1186/s13287-023-03285-9
Development and validation of a glioma-associated mesenchymal stem cell-related gene prognostic index for predicting prognosis and guiding individualized therapy in glioma
Abstract
Background: Recent studies have demonstrated that glioma-associated mesenchymal stem cells (GA-MSCs) are implicated in the regulation of glioma malignant progression. However, the prognostic value of GA-MSCs has not been comprehensively explored in glioma.
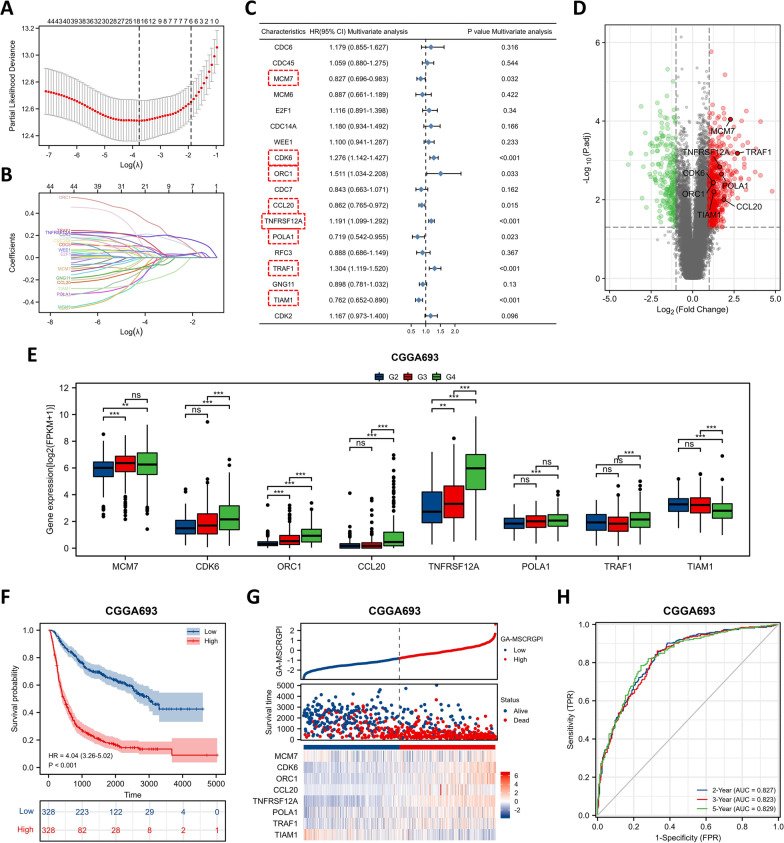
Methods: We extracted GA-MSCs from glioma tissues, established intracranial xenograft models in nude mice, and obtained GA-MSC-related genes (GA-MSCRGs) by using microarrays. The transcriptome data and clinical information of glioma patients were obtained from the CGGA and TCGA databases. We screened 8 prognostic GA-MSCRGs to construct a prognostic index by using the multivariate Cox regression method. The validity of the GA-MSCRGPI was verified in the training (CGGA693) and validation (TCGA and CGGA325) cohorts. The expression patterns of these 8 GA-MSCRGs were validated in 78 glioma tissue specimens by using a qRT‒PCR assay.
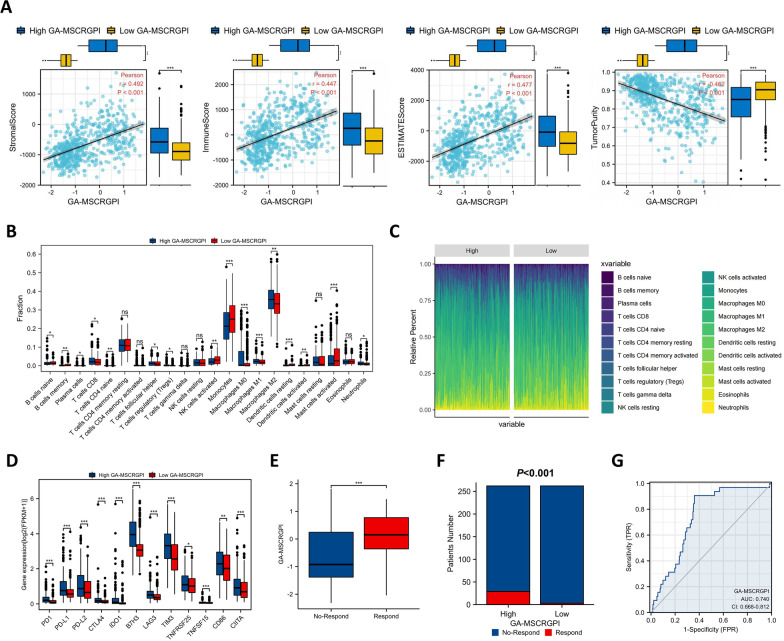
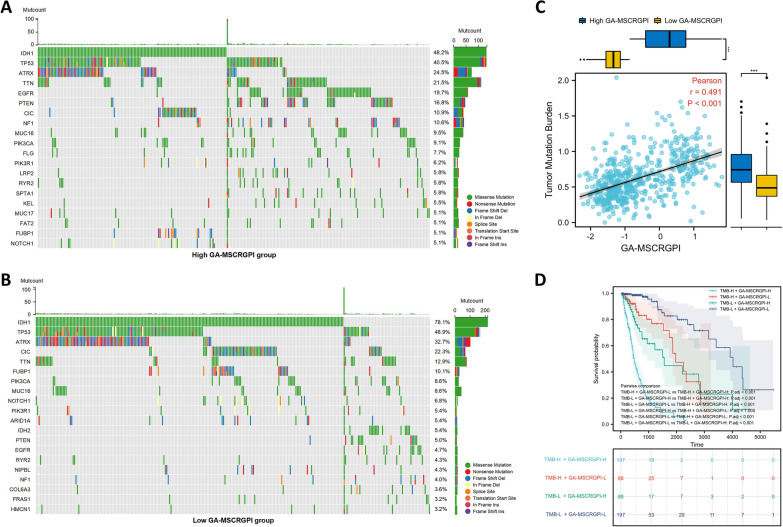
Results: GA-MSCs were successfully isolated from glioma tissues. Based on intracranial xenograft models and transcriptome microarray screening, 8 genes (MCM7, CDK6, ORC1, CCL20, TNFRSF12A, POLA1, TRAF1 and TIAM1) were selected for the construction of a GA-MSC-related gene prognostic index (GA-MSCRGPI). In both the training and validation cohorts, high GA-MSCRGPI patients showed an inferior survival outcome compared with low GA-MSCRGPI patients. A nomogram was established based on independent prognostic indicators (age, WHO grade and GA-MSCRGPI) and exhibited a strong forecasting ability for overall survival (OS). Moreover, we found that the GA-MSCRGPI could evaluate the prognosis of glioma patients undergoing chemoradiotherapy. The high GA-MSCRGPI group exhibited higher immune, stromal and ESTIMATE scores; lower tumor purity; higher infiltration of Tregs and M2-type macrophages; fewer activated NK cells; and higher expression of immune checkpoints. Tumor Immune Dysfunction and Exclusion (TIDE) showed that the high GA-MSCRGPI group had more responders to ICI therapy. The results of the genetic mutation profile and tumor mutation burden (TMB) in different GA-MSCRGPI subgroups further supplement GA-MSCRGPI-related mechanisms. Finally, the expression patterns of 8 selected GA-MSCRGs in GA-MSCRGPI were correlated with glioma WHO grades to a certain extent.
Conclusion: The constructed GA-MSCRGPI could predict prognosis and guide individualized therapy in glioma patients.
Keywords: Chemoradiotherapy; Genomic alterations; Glioma; Glioma-associated mesenchymal stem cells; Immune microenvironment; Immunotherapy; Prognosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Nicholson JG, Fine HA. Diffuse glioma heterogeneity and its therapeutic implications. Cancer Discov. 2021;11:575–590. doi: 10.1158/2159-8290.CD-20-1474. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
