

CT appearances and classification of hepatic epithelioid hemangioendothelioma
- PMID: 37005950
- PMCID: PMC10067783
- DOI: 10.1186/s13244-023-01410-z
CT appearances and classification of hepatic epithelioid hemangioendothelioma
Abstract
Background: Hepatic epithelioid hemangioendothelioma (HEH) is extremely rare, and CT features have never been analyzed in a large group of patients.
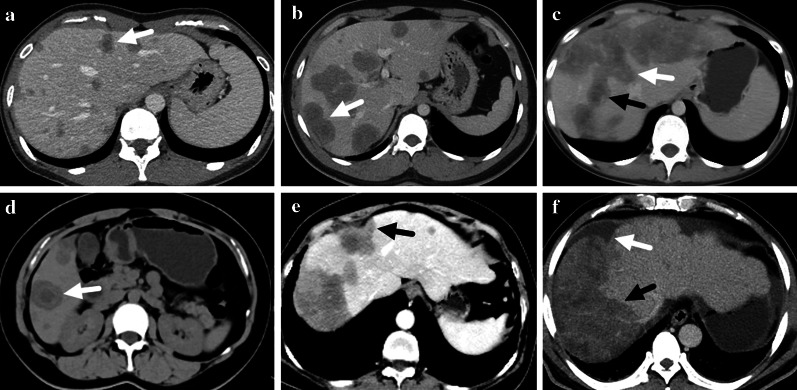
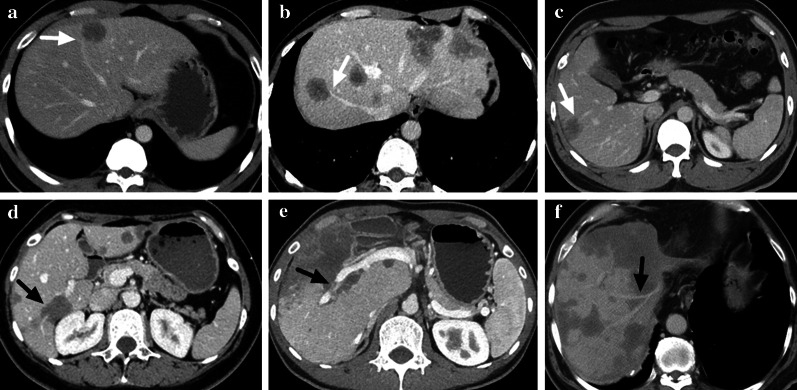
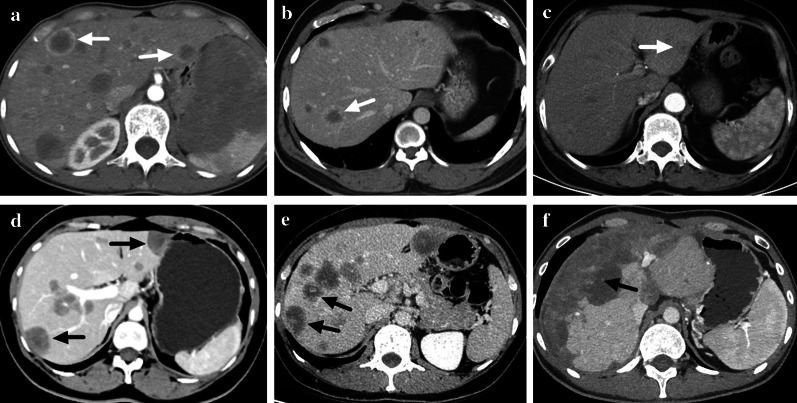
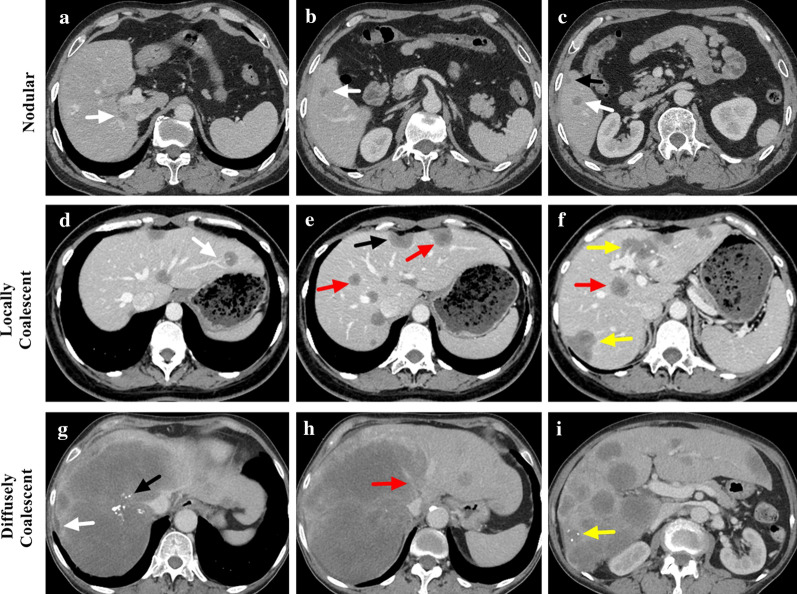
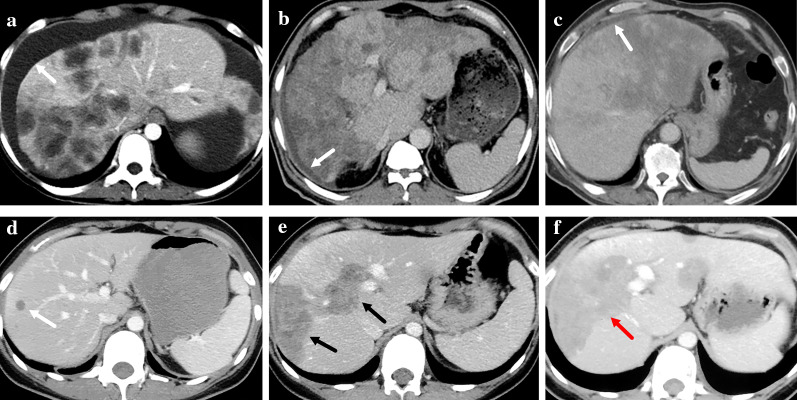
Methods: A retrospective study was designed to review the contrast-enhanced CT images of HEH patients. Intrahepatic lesions were categorized into three types: nodular, locally coalescent (coalescent lesion contained in one segment) or diffusely coalescent (coalescent lesion occupied more than one segment). CT features were compared among lesions of different sizes and patients with different lesion types.
Results: A total of 93 HEH patients were included in this study, and 740 lesions were analyzed. The results of per-lesion analysis showed that medium lesions (2-5 cm) had the highest rate of lollipop sign (16.8%) and target-like enhancement (43.1%), while lesions in large group (> 5 cm) had the highest rate of capsular retraction (38.8%) and vascular invasion (38.8%). The differences on enhancement pattern and the rates of lollipop sign and capsular retraction were significant among lesions of different sizes (p < 0.001, respectively). The results of per-patient analysis showed that patients in locally coalescent group had the highest rates of lollipop sign (74.3%) and target sign (94.3%). All patients in diffusely coalescent group had capsular retraction and vascular invasion. CT appearances of capsular retraction, lollipop sign, target sign and vascular invasion differed significantly among patients with different lesion types (p < 0.001, p = 0.005, p = 0.006 and p < 0.001, respectively).
Conclusion: CT features variated among HEH patients with different lesion types, and radiological appearances of HEH should be classified into nodular type, locally coalescent type and diffusely coalescent type.
Keywords: CT; Hepatic epithelioid hemangioendothelioma; Hepatic tumors; Rare liver tumors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Liu XL, Yang ZY. Outcomes of hepatic epithelioid hemangioendothelioma with different managements: a retrospective investigation. Eur Rev Med Pharmacol Sci. 2021;25(12):4274–4282. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
