

Early outcomes of "low-risk" patients undergoing lung resection assessed by cardiopulmonary exercise testing: Single-institution experience
- PMID: 37009610
- PMCID: PMC10062454
- DOI: 10.3389/fsurg.2023.1130919
Early outcomes of "low-risk" patients undergoing lung resection assessed by cardiopulmonary exercise testing: Single-institution experience
Abstract
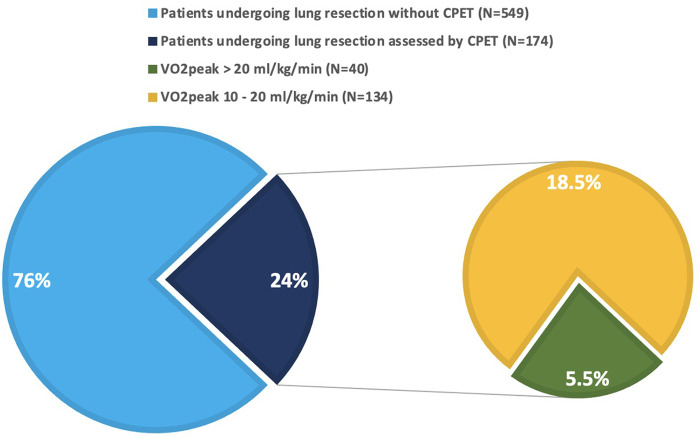
Objective: Cardiopulmonary exercise testing (CPET) is currently recommended for all patients undergoing lung resection with either respiratory comorbidities or functional limitations. The main parameter evaluated is oxygen consumption at peak (VO2peak). Patients with VO2peak above 20 ml/kg/min are classified as low risk surgical candidates. The aims of this study were to evaluate postoperative outcomes of low-risk patients, and to compare their outcomes with those of patients without pulmonary impairment at respiratory function testing.
Methods: Retrospective monocentric observational study was designed, evaluating outcomes of patients undergoing lung resection at San Paolo University Hospital, Milan, Italy, between January 2016 and November 2021, preoperatively assessed by CPET, according to 2009 ERS/ESTS guidelines. All low-risk patients undergoing any extent surgical lung resection for pulmonary nodules were enrolled. Postoperative major cardiopulmonary complications or death, occurring within 30 days from surgery, were assessed. A case-control study was nested, matching 1:1 for type of surgery the cohort population with control patients without functional respiratory impairment consecutively undergoing surgery at the same centre in the study period.
Results: A total of 80 patients were enrolled: 40 subjects were preoperatively assessed by CPET and deemed at low risk, whereas 40 subjects represented the control group. Among the first, 4 patients (10%) developed major cardiopulmonary complications, and 1 patient (2.5%) died within 30 days from surgery. In the control group, 2 patients (5%) developed complications and none of the patients (0%) died. The differences in morbidity and mortality rates did not reach statistically significance. Instead, age, weight, BMI, smoking history, COPD incidence, surgical approach, FEV1, Tiffenau, DLCO and length of hospital stay resulted significantly different between the two groups. At a case-by-case analysis, CPET revealed a pathological pattern in each complicated patient, in spite of VO2peak above target for safe surgery.
Conclusions: Postoperative outcomes of low-risk patients undergoing lung resections are comparable to those of patients without any pulmonary functional impairment; nonetheless the formers represent a dramatically different category of individuals from the latter and may harbour few patients with worse outcomes. CPET variables overall interpretation may add to the VO2peak in identifying higher risk patients, even in this subgroup.
Keywords: VO2peak; cardiopulmonary complications; cardiopulmonary exercise testing (CPET); peak oxygen uptake; postoperative outcomes; thoracic surgery.
© 2023 Orlandi, Rinaldo, Mazzucco, Baccelli, Mondoni, Marchetti, Zagaria, Cefalo, Leporati, Montoli, Ghilardi, Baisi and Centanni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: diagnosis and management of lung cancer, 3rd ed: american college of chest physicians evidence-based clinical practice guidelines. Chest. (2013) 143(5 Suppl):e166S–90S. 10.1378/chest.12-2395 - DOI - PubMed