

Assessment of the inferior vena cava collapsibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on healthy volunteers
- PMID: 37009935
- PMCID: PMC10068684
- DOI: 10.1186/s40635-023-00505-7
Assessment of the inferior vena cava collapsibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on healthy volunteers
Abstract
Purpose: Assessment of the inferior vena cava (IVC) respiratory variation may be clinically useful for the estimation of fluid-responsiveness and venous congestion; however, imaging from subcostal (SC, sagittal) region is not always feasible. It is unclear if coronal trans-hepatic (TH) IVC imaging provides interchangeable results. The use of artificial intelligence (AI) with automated border tracking may be helpful as part of point-of-care ultrasound but it needs validation.
Methods: Prospective observational study conducted in spontaneously breathing healthy volunteers with assessment of IVC collapsibility (IVCc) in SC and TH imaging, with measures taken in M-mode or with AI software. We calculated mean bias and limits of agreement (LoA), and the intra-class correlation (ICC) coefficient with their 95% confidence intervals.
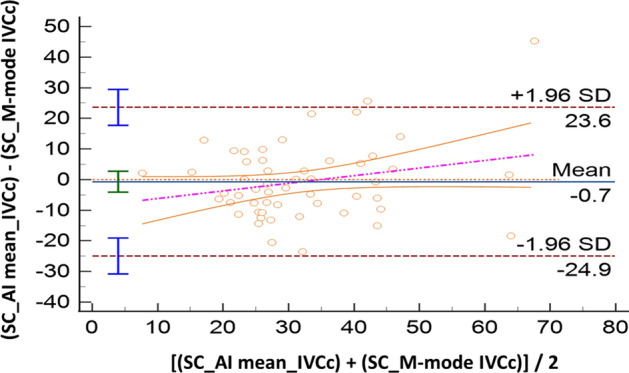
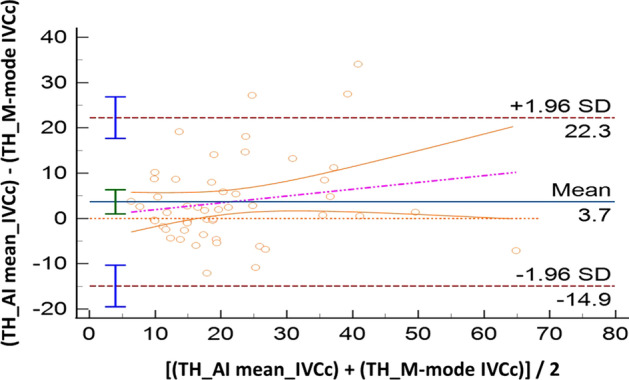
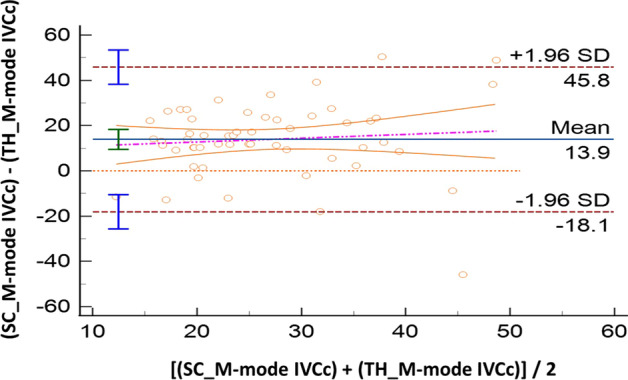
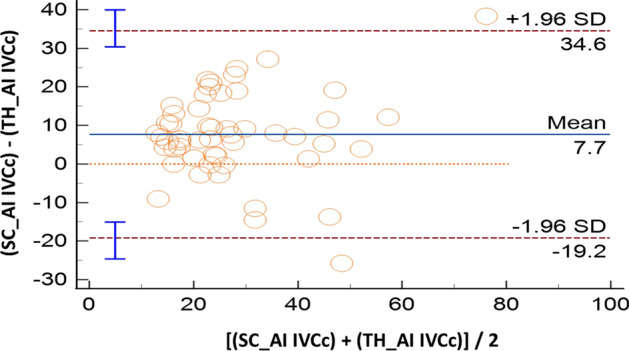
Results: Sixty volunteers were included; IVC was not visualized in five of them (n = 2, both SC and TH windows, 3.3%; n = 3 in TH approach, 5%). Compared with M-mode, AI showed good accuracy both for SC (IVCc: bias - 0.7%, LoA [- 24.9; 23.6]) and TH approach (IVCc: bias 3.7%, LoA [- 14.9; 22.3]). The ICC coefficients showed moderate reliability: 0.57 [0.36; 0.73] in SC, and 0.72 [0.55; 0.83] in TH. Comparing anatomical sites (SC vs TH), results produced by M-mode were not interchangeable (IVCc: bias 13.9%, LoA [- 18.1; 45.8]). When this evaluation was performed with AI, such difference became smaller: IVCc bias 7.7%, LoA [- 19.2; 34.6]. The correlation between SC and TH assessments was poor for M-mode (ICC = 0.08 [- 0.18; 0.34]) while moderate for AI (ICC = 0.69 [0.52; 0.81]).
Conclusions: The use of AI shows good accuracy when compared with the traditional M-mode IVC assessment, both for SC and TH imaging. Although AI reduces differences between sagittal and coronal IVC measurements, results from these sites are not interchangeable.
Keywords: Critical care; Inferior vena cava; Subcostal; Transhepatic; Ultrasound.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Sanfilippo F, Messina A, Cecconi M, Astuto M (2020) Ten answers to key questions for fluid management in intensive care. Medicina intensiva - PubMed
-
- Sanfilippo F, Scolletta S (2017) Fluids in cardiac surgery: sailing calm on a stormy sea? Common sense is the guidance. Minerva anestesiologica - PubMed
LinkOut - more resources
Full Text Sources
Medical
