

Predictors for selective flexure mobilization during robotic anterior resection for rectal cancer: a prospective cohort analysis
- PMID: 37010604
- PMCID: PMC10322756
- DOI: 10.1007/s00464-023-10008-x
Predictors for selective flexure mobilization during robotic anterior resection for rectal cancer: a prospective cohort analysis
Abstract
Introduction: Splenic flexure mobilization (SFM) may be indicated during anterior resection to provide a tension-free anastomosis. However, to date, no score allows identifying patients who may benefit from SFM.
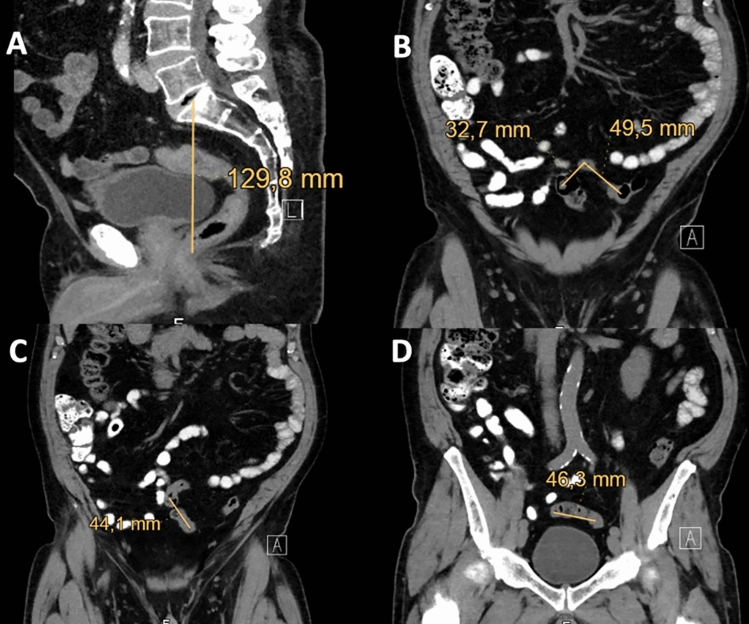
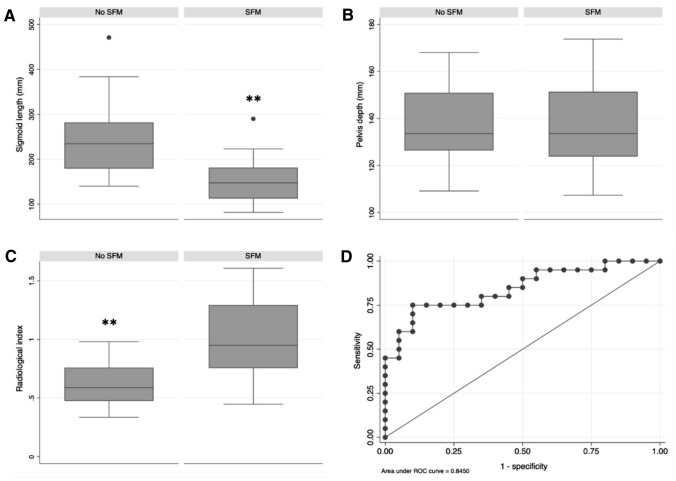
Methods: Patients who underwent robotic anterior resection for rectal cancer were identified from a prospective register. Demographic and cancer-related variables were extracted, and predictors of SFM were identified using regression models. Thereafter, 20 patients with SFM and 20 patients without SFM were randomly selected and their pre-operative CTscan were reviewed. The radiological index was defined as 1/(sigmoid length/pelvis depth). The optimal cut-off value for predicting SFM was identified using ROC curve analysis.
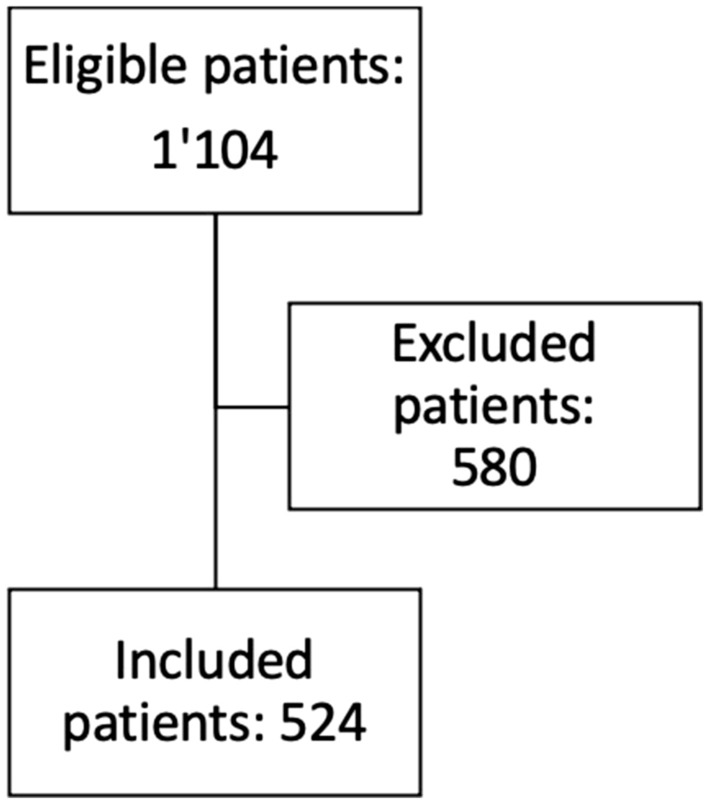
Results: Five hundred and twenty-four patients were included. SFM was performed in 121 patients (27.8%) and increased operative time by 21.8 min (95% CI: 11.3 to 32.4, p < 0.001). The incidence of postoperative complications did not differ between patient with or without SFM. Realization of an anastomosis was the main predictor for SFM (OR: 42.4, 95% CI: 5.8 to 308.5, p < 0.001). In patients with colorectal anastomosis, both sigmoid length (15 ± 5.1 cm versus 24.2 ± 80.9 cm, p < 0.001) and radiological index (1 ± 0.3 versus 0.6 ± 0.2, p < 0.001) differed between patients who had SFM and patients who did not. ROC curve analysis of the radiological index indicated an optimal cut-off value of 0.8 (sensitivity: 75%, specificity: 90%).
Conclusion: SFM was performed in 27.8% of patients who underwent robotic anterior resection, and increased operative time by 21.8 min. For optimal surgical planning, patients requiring SFM can be identified based on pre-operative CT using the index 1/(sigmoid length/pelvis depth) with a cut-off value set at 0.8.
Keywords: Da Vinci; LAR; Low anterior resection; Robotics; TME; Total mesorectum excision.
© 2023. The Author(s).
Conflict of interest statement
Dr. Jeremy Meyer, Dr. George van der Schelling, Dr. Jan Wijsman, Prof. Frédéric Ris and Dr. Rogier Crolla have no conflict of interest to disclose related to the present manuscript.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
