

Neuroimaging of hypophysitis: etiologies and imaging mimics
- PMID: 37010787
- PMCID: PMC10468747
- DOI: 10.1007/s11604-023-01417-y
Neuroimaging of hypophysitis: etiologies and imaging mimics
Abstract
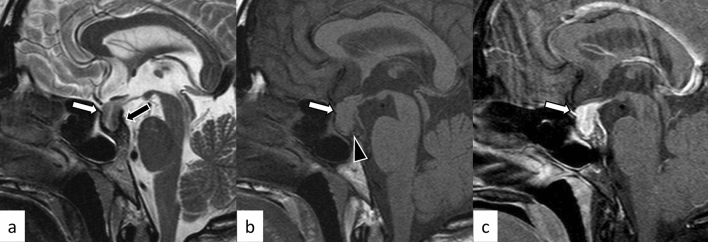
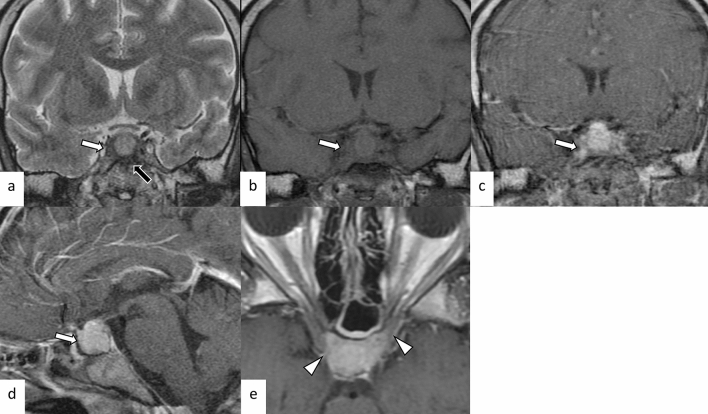
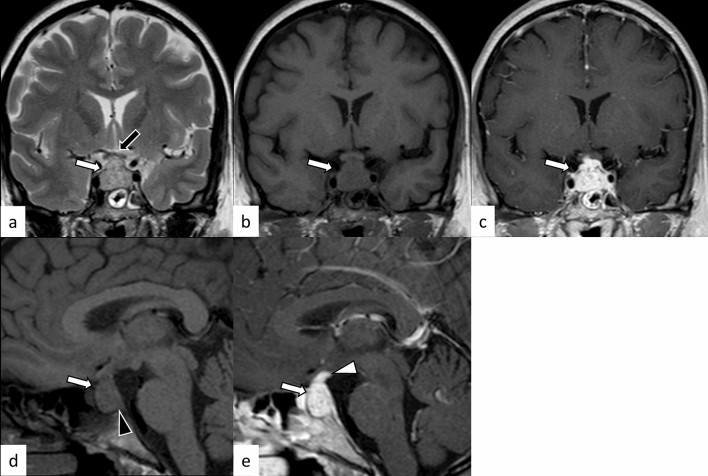
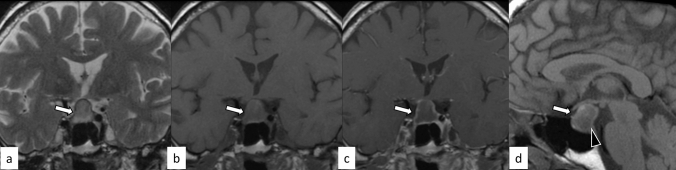
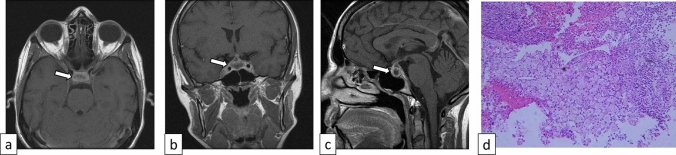
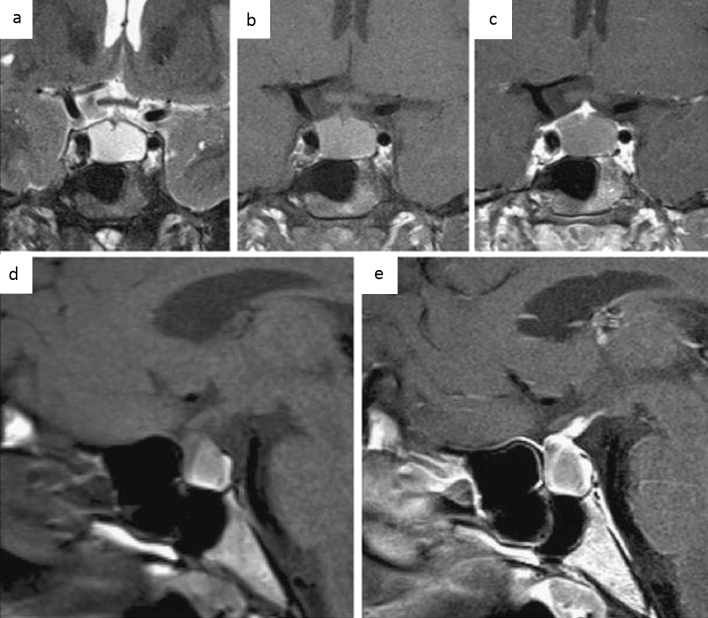
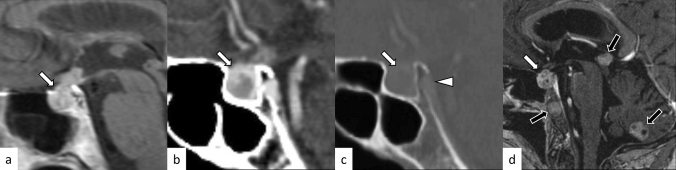
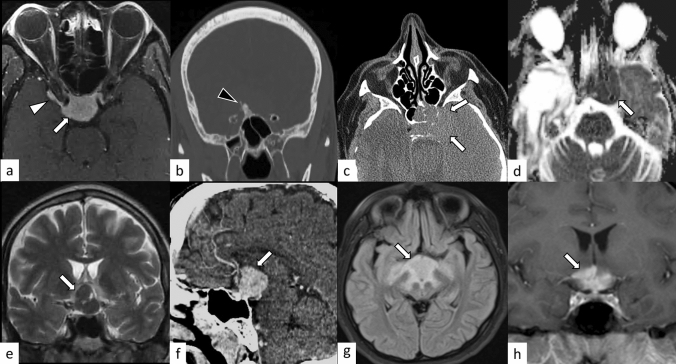
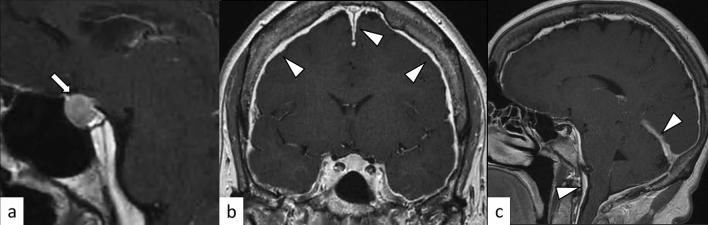
Hypophysitis is an inflammatory disease affecting the pituitary gland. Hypophysitis can be classified into multiple types depending on the mechanisms (primary or secondary), histology (lymphocytic, granulomatous, xanthomatous, plasmacytic/IgG4 related, necrotizing, or mixed), and anatomy (adenohypophysitis, infundibulo-neurohypophysitis, or panhypophysitis). An appropriate diagnosis is vital for managing these potentially life-threatening conditions. However, physiological morphological alterations, remnants, and neoplastic and non-neoplastic lesions may masquerade as hypophysitis, both clinically and radiologically. Neuroimaging, as well as imaging findings of other sites of the body, plays a pivotal role in diagnosis. In this article, we will review the types of hypophysitis and summarize clinical and imaging features of both hypophysitis and its mimickers.
Keywords: Hypophysitis; Magnetic resonance imaging; PitNET.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures











References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
