

Intravenous to Oral Antibiotic Switch Therapy Among Patients Hospitalized With Community-Acquired Pneumonia
- PMID: 37011018
- PMCID: PMC10527888
- DOI: 10.1093/cid/ciad196
Intravenous to Oral Antibiotic Switch Therapy Among Patients Hospitalized With Community-Acquired Pneumonia
Abstract
Background: Community-acquired pneumonia (CAP) is a leading cause of hospital admissions and antimicrobial use. Clinical practice guidelines recommend switching from intravenous (IV) to oral antibiotics once patients are clinically stable.
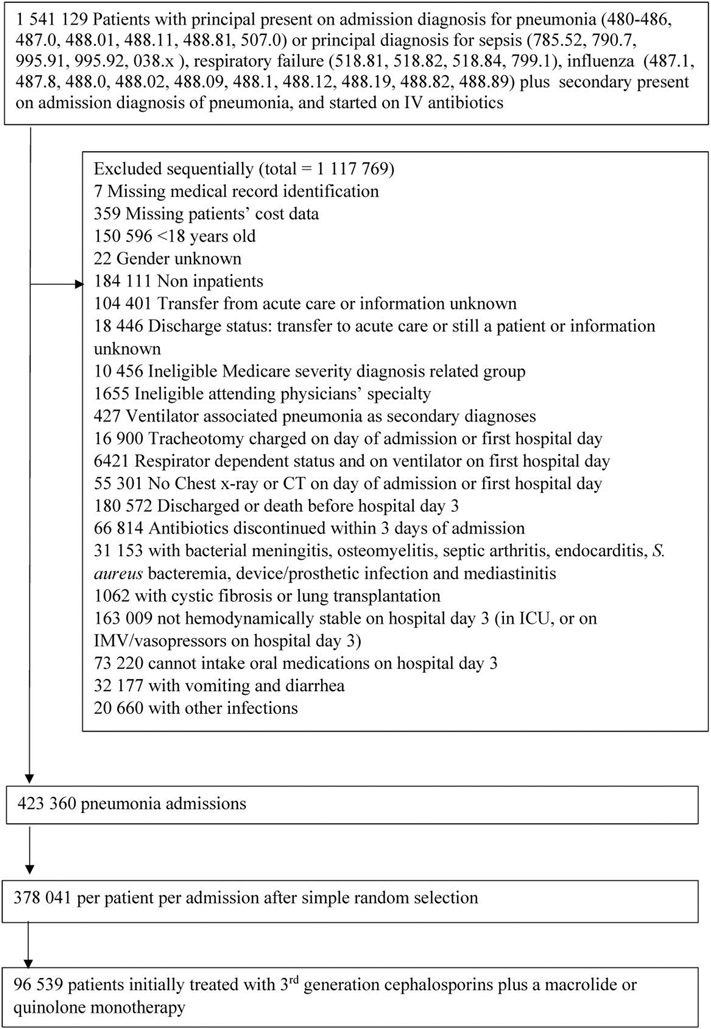
Methods: We conducted a retrospective cohort study of adults admitted with CAP and initially treated with IV antibiotics at 642 US hospitals from 2010 through 2015. Switching was defined as discontinuation of IV and initiation of oral antibiotics without interrupting therapy. Patients switched by hospital day 3 were considered early switchers. We compared length of stay (LOS), in-hospital 14-day mortality, late deterioration (intensive care unit [ICU] transfer), and hospital costs between early switchers and others, controlling for hospital characteristics, patient demographics, comorbidities, initial treatments, and predicted mortality.
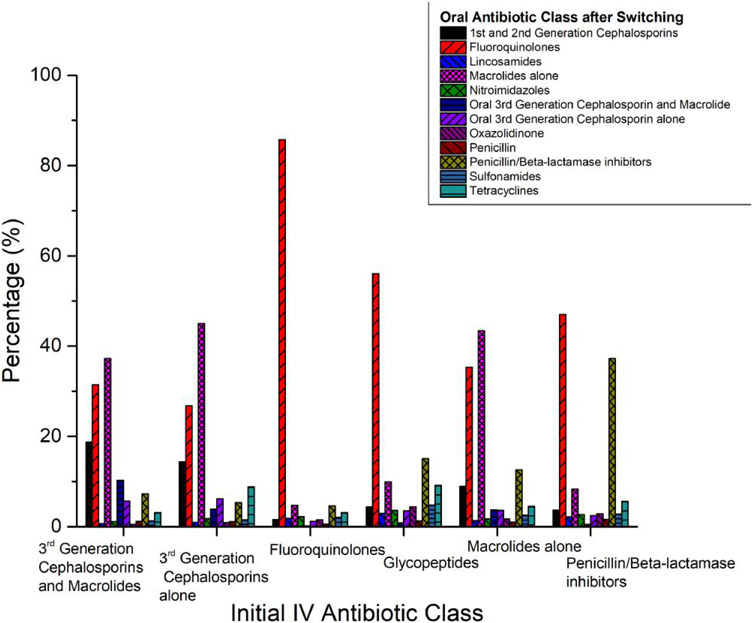
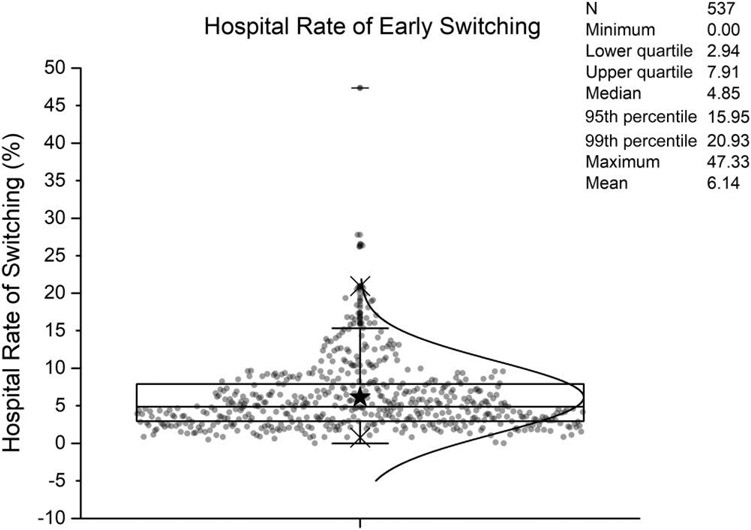
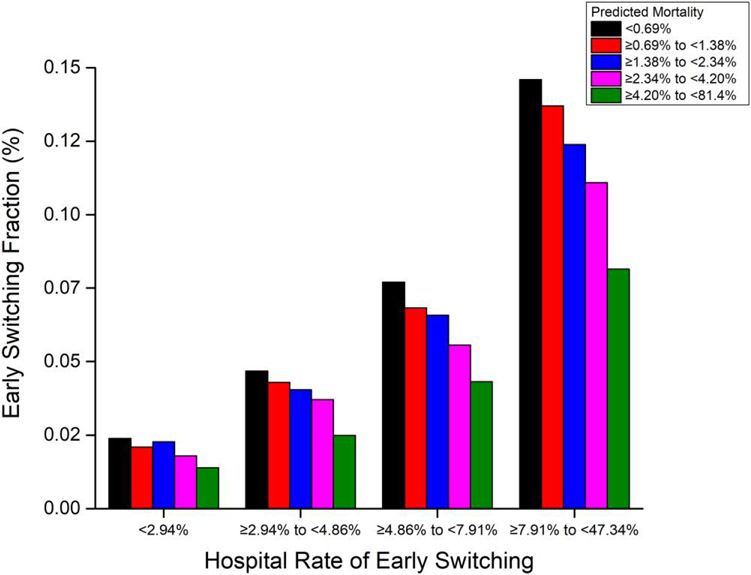
Results: Of 378 041 CAP patients, 21 784 (6%) were switched early, most frequently to fluoroquinolones. Patients switched early had fewer days on IV antibiotics, shorter duration of inpatient antibiotic treatment, shorter LOS, and lower hospitalization costs, but no significant excesses in 14-day in-hospital mortality or late ICU admission. Patients at a higher mortality risk were less likely to be switched. However, even in hospitals with relatively high switch rates, <15% of very low-risk patients were switched early.
Conclusions: Although early switching was not associated with worse outcomes and was associated with shorter LOS and fewer days on antibiotics, it occurred infrequently. Even in hospitals with high switch rates, <15% of very low-risk patients were switched early. Our findings suggest that many more patients could be switched early without compromising outcomes.
Keywords: IV to oral; antimicrobial stewardship; community-acquired pneumonia; switch therapy.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest. A. D. reports research funding (to institution) from the Clorox Company, consultant fees from Merck, and grants or contracts to institution, unrelated to the current study, from Seres Therapeutics. M. K. reports royalties from UpToDate and grants or contracts to institution from the Centers for Disease Control and Prevention and the Agency for Healthcare Research and Quality. M. D. Z. reports research support from Tetraphase Pharmaceuticals, Astellas, Lungpacer, Merck, Spero, Medicines Co, Melinta, scPharma, Shionogi, and Pfizer; consulting fees from Paratek, Arasanis, Shionogi, Pfizer, Nabriva, scPharma, and Melinta; and stock or stock options from Johnson & Johnson. T. H. reports consulting fees from the Cerner Corporation. P. B. I. reports consulting fees from Colgate-Palmolive. S. H. reports a role with the Society for Health Epidemiology of America (councilor, board of trustees, volunteer; no compensation). All remaining authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Williams S, Gousen S, DeFrances C. National Hospital Care Survey demonstration projects: pneumonia inpatient hospitalizations and emergency department visits. Natl Health Stat Report 2018; 116:1–11. - PubMed
-
- Brown K, Valenta K, Fisman D, Simor A, Daneman N. Hospital ward antibiotic prescribing and the risks of Clostridium difficile infection. JAMA Intern Med 2015; 175:626–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
