

Challenges of acute febrile illness diagnosis in a national infectious diseases center in Rio de Janeiro: 16-year experience of syndromic surveillance
- PMID: 37011087
- PMCID: PMC10101631
- DOI: 10.1371/journal.pntd.0011232
Challenges of acute febrile illness diagnosis in a national infectious diseases center in Rio de Janeiro: 16-year experience of syndromic surveillance
Abstract
Introduction: Acute febrile illnesses (AFI) are a frequent chief complaint in outpatients. Because the capacity to investigate the causative pathogen of AFIs is limited in low- and middle-income countries, patient management may be suboptimal. Understanding the distribution of causes of AFI can improve patient outcomes. This study aims to describe the most common etiologies diagnosed over a 16-years period in a national reference center for tropical diseases in a large urban center in Rio de Janeiro, Brazil.
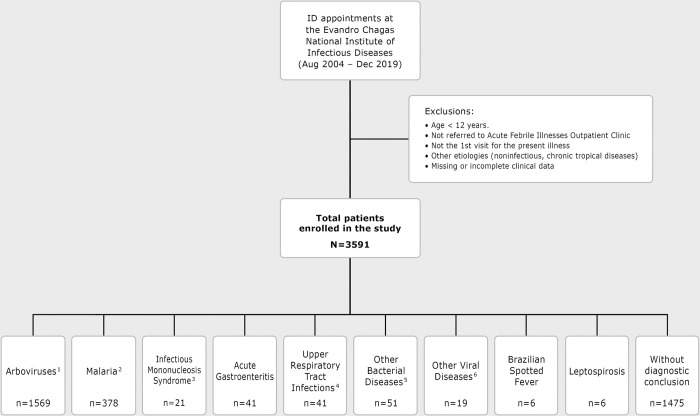
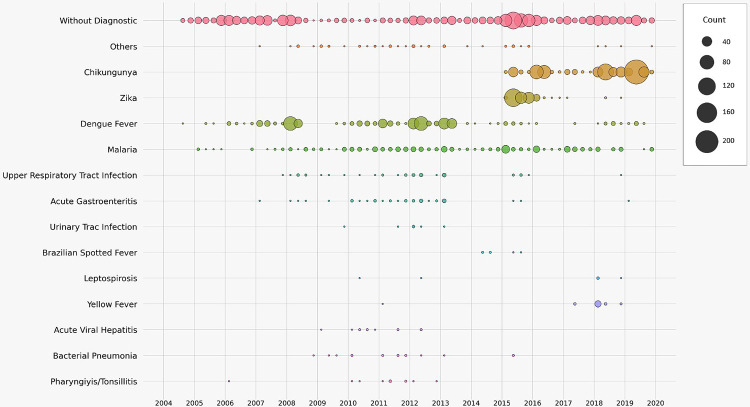
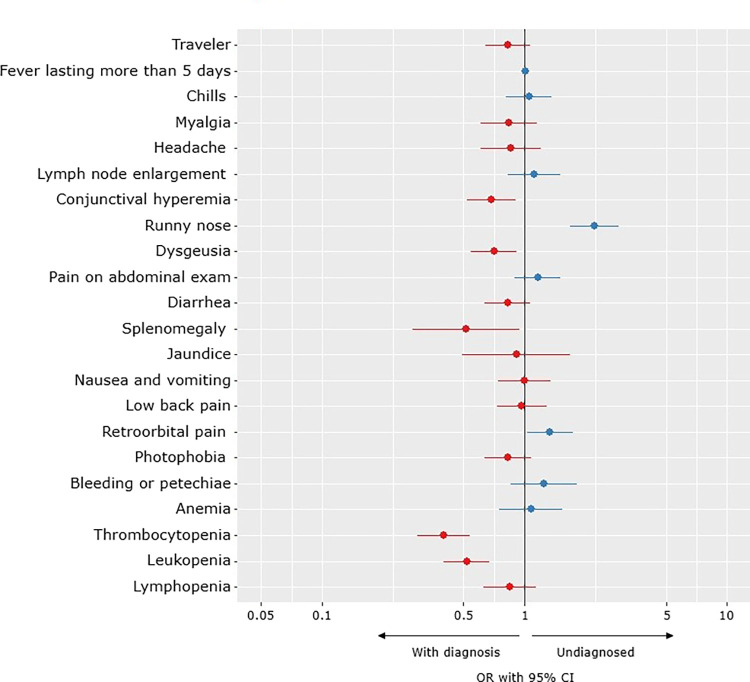
Methods: From August 2004-December 2019, 3591 patients > 12 years old, with AFI and/or rash were eligible. Complementary exams for etiological investigation were requested using syndromic classification as a decision guide. Results. Among the 3591 patients included, endemic arboviruses such as chikungunya (21%), dengue (15%) and zika (6%) were the most common laboratory-confirmed diagnosis, together with travel-related malaria (11%). Clinical presumptive diagnosis lacked sensitivity for emerging diseases such as zika (31%). Rickettsia disease and leptospirosis were rarely investigated and an infrequent finding when based purely on clinical features. Respiratory symptoms increased the odds for the diagnostic remaining inconclusive.
Conclusions: Numerous patients did not have a conclusive etiologic diagnosis. Since syndromic classification used for standardization of etiological investigation and presumptive clinical diagnosis had moderate accuracy, it is necessary to incorporate new diagnostic technologies to improve diagnostic accuracy and surveillance capacity.
Copyright: © 2023 Bressan et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lamas C, Favacho A, Rozental T, Bóia MN, Kirsten AH, Guterres A, et al. Characterization of rickettsia rickettsii in a case of Fatal Brazilian spotted fever in the city of Rio de Janeiro, Brazil. Braz J Infect Dis 2008; 12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
