

Surgical polarimetric endoscopy for the detection of laryngeal cancer
- PMID: 37012312
- PMCID: PMC10427430
- DOI: 10.1038/s41551-023-01018-0
Surgical polarimetric endoscopy for the detection of laryngeal cancer
Erratum in
-
Publisher Correction: Surgical polarimetric endoscopy for the detection of laryngeal cancer.Nat Biomed Eng. 2023 Aug;7(8):1053. doi: 10.1038/s41551-023-01063-9. Nat Biomed Eng. 2023. PMID: 37291436 Free PMC article. No abstract available.
Abstract
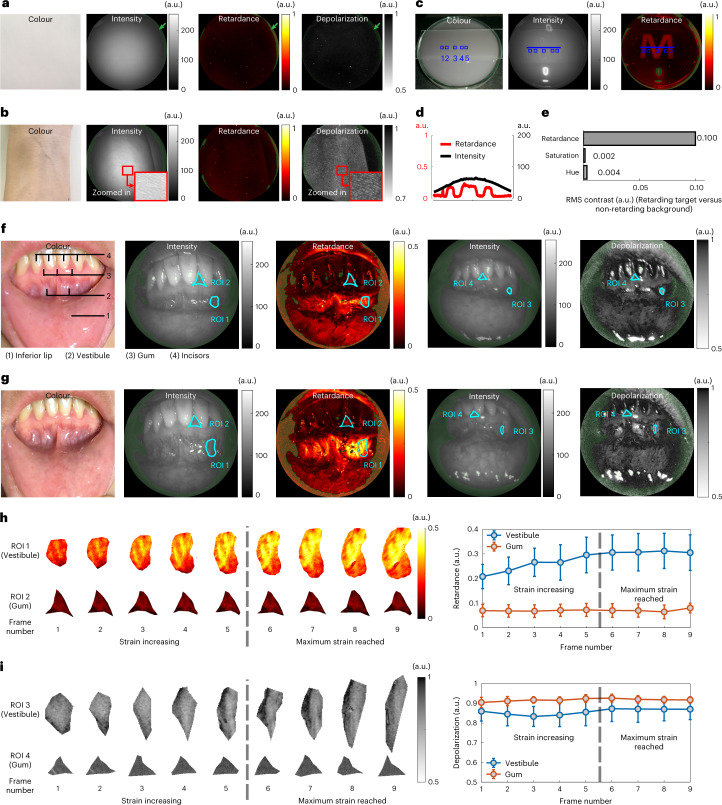
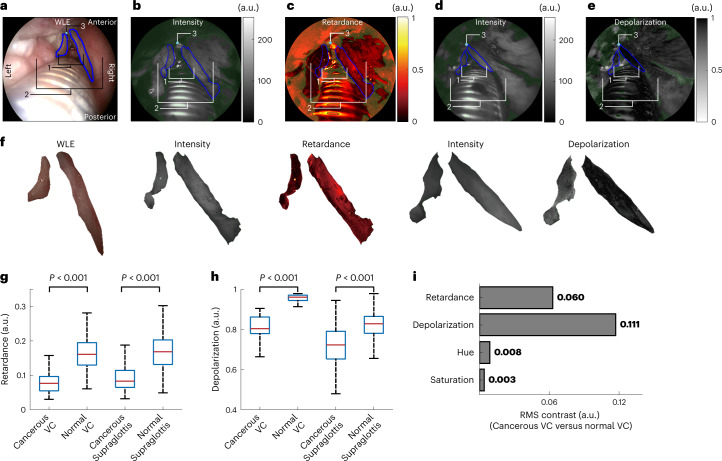
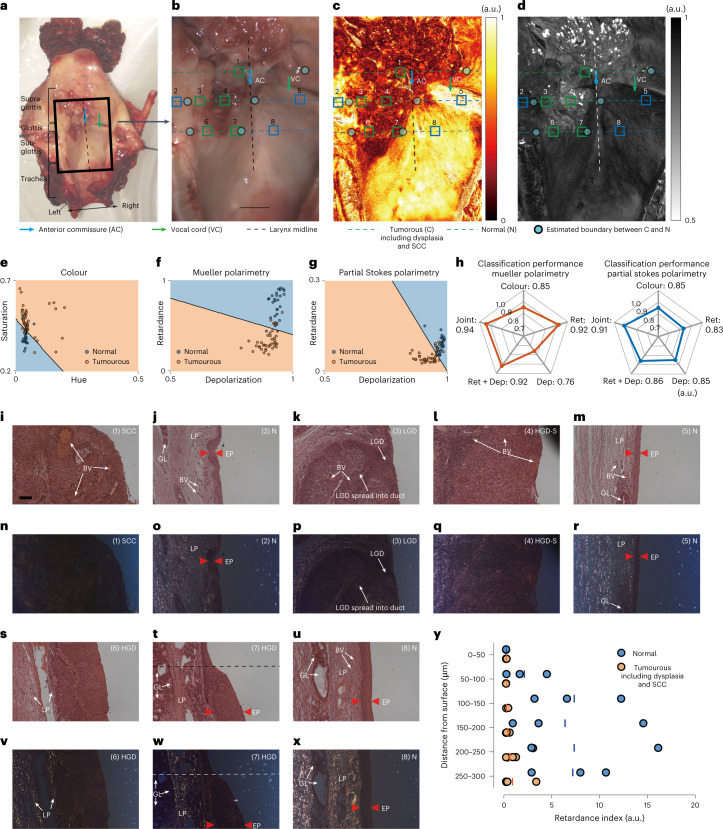
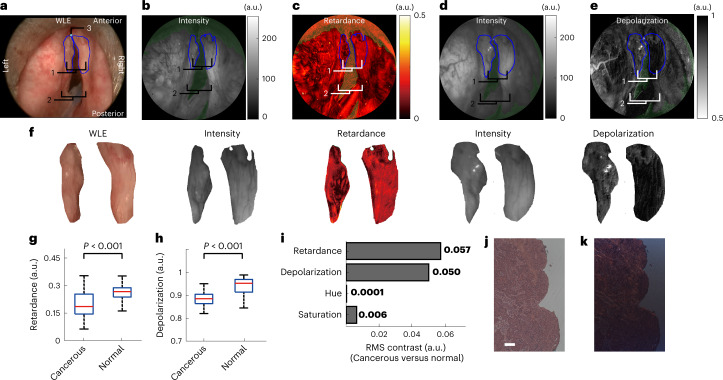
The standard-of-care for the detection of laryngeal pathologies involves distinguishing suspicious lesions from surrounding healthy tissue via contrasts in colour and texture captured by white-light endoscopy. However, the technique is insufficiently sensitive and thus leads to unsatisfactory rates of false negatives. Here we show that laryngeal lesions can be better detected in real time by taking advantage of differences in the light-polarization properties of cancer and healthy tissues. By measuring differences in polarized-light retardance and depolarization, the technique, which we named 'surgical polarimetric endoscopy' (SPE), generates about one-order-of-magnitude greater contrast than white-light endoscopy, and hence allows for the better discrimination of cancerous lesions, as we show with patients diagnosed with squamous cell carcinoma. Polarimetric imaging of excised and stained slices of laryngeal tissue indicated that changes in the retardance of polarized light can be largely attributed to architectural features of the tissue. We also assessed SPE to aid routine transoral laser surgery for the removal of a cancerous lesion, indicating that SPE can complement white-light endoscopy for the detection of laryngeal cancer.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Riu Pons F, et al. Narrow-band imaging and high-definition white-light endoscopy in patients with serrated lesions not fulfilling criteria for serrated polyposis syndrome: a randomized controlled trial with tandem colonoscopy. BMC Gastroenterol. 2020;20:111. doi: 10.1186/s12876-020-01257-4. - DOI - PMC - PubMed
-
- Menon S, Dhar A, Hoare J, Trudgill N. How commonly is gastric cancer missed at endoscopy: a UK primary care based study. Gut. 2012;61:A43. doi: 10.1136/gutjnl-2012-302514a.98. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
