

The genetic landscape and clinical implication of pediatric Moyamoya angiopathy in an international cohort
- PMID: 37012328
- PMCID: PMC10325976
- DOI: 10.1038/s41431-023-01320-0
The genetic landscape and clinical implication of pediatric Moyamoya angiopathy in an international cohort
Abstract
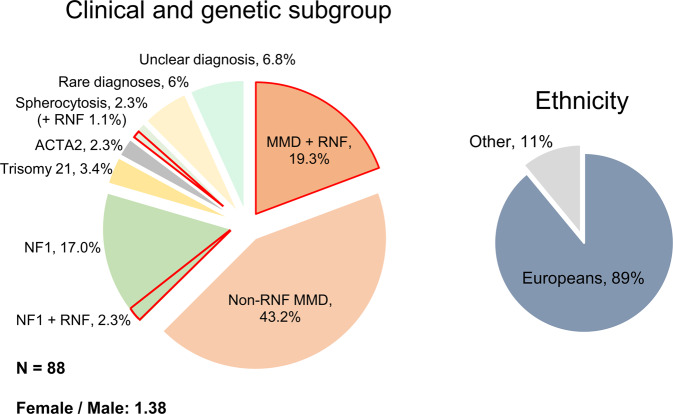
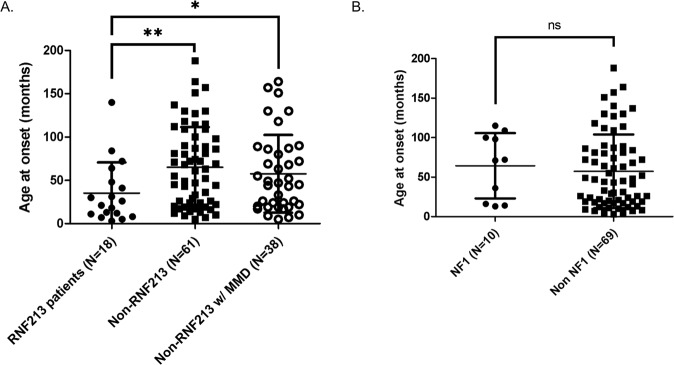
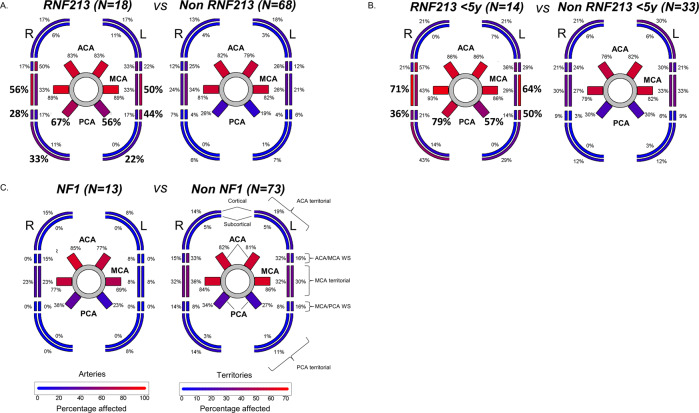
Pediatric Moyamoya Angiopathy (MMA) is a progressive intracranial occlusive arteriopathy that represents a leading cause of transient ischemic attacks and strokes in childhood. Despite this, up to now no large, exclusively pediatric MMA cohort has been subjected to systematic genetic investigation. In this study, we performed molecular karyotyping, exome sequencing and automated structural assessment of missense variants on a series of 88 pediatric MMA patients and correlated genetic, angiographic and clinical (stroke burden) findings. The two largest subgroups in our cohort consisted of RNF213 and neurofibromatosis type 1 (NF1) patients. While deleterious RNF213 variants were associated with a severe MMA clinical course with early symptom onset, frequent posterior cerebral artery involvement and higher stroke rates in multiple territories, NF1 patients had a similar infarct burden compared to non-NF1 individuals and were often diagnosed incidentally during routine MRIs. Additionally, we found that MMA-associated RNF213 variants have lower predicted functional impact compared to those associated with aortic disease. We also raise the question of MMA as a feature of recurrent as well as rare chromosomal imbalances and further support the possible association of MMA with STAT3 deficiency. In conclusion, we provide a comprehensive characterization at the genetic and clinical level of a large exclusively pediatric MMA population. Due to the clinical differences found across genetic subgroups, we propose genetic testing for risk stratification as part of the routine assessment of pediatric MMA patients.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Uncovering the genetic architecture of paediatric moyamoya angiopathy: implications for disease pathogenesis.Eur J Hum Genet. 2023 Jul;31(7):733-734. doi: 10.1038/s41431-023-01353-5. Epub 2023 Apr 5. Eur J Hum Genet. 2023. PMID: 37020136 Free PMC article. No abstract available.
-
Investigation and management of pediatric moyamoya arteriopathy in the era of genotype-phenotype correlation studies.Eur J Hum Genet. 2023 Jul;31(7):735-737. doi: 10.1038/s41431-023-01369-x. Epub 2023 May 15. Eur J Hum Genet. 2023. PMID: 37188827 Free PMC article. No abstract available.
References
-
- Kleinloog, R, Regli, L, Rinkel, GJE, Klijn, CJM. Regional differences in incidence and patient characteristics of moyamoya disease: a systematic review. J Neurol Neurosurg Psychiatry. 2012;83:531–6. http://jnnp.bmj.com/. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
