

doi: 10.1016/j.eats.2022.11.021.
eCollection 2023 Mar.
Anterior Shoulder Instability Treated Through an Anterior Arthroscopic Approach
Affiliations
- PMID: 37013020
- PMCID: PMC10066418
- DOI: 10.1016/j.eats.2022.11.021
Item in Clipboard
Anterior Shoulder Instability Treated Through an Anterior Arthroscopic Approach
Arthrosc Tech.
.
Abstract
Anterior shoulder instability remains one of the main indications for shoulder surgery. We present a modified way of treating anterior shoulder instability in the beach-chair position from an anterior arthroscopic approach through the rotator interval. This technique opens the rotator interval, which increases the working area and allows us to work without cannulae. Through this approach, we can treat all injuries comprehensively and, if necessary, switch to other arthroscopic techniques used for instability such as arthroscopic Latarjet or anterior ligamentoplasties.
© 2022 The Authors.
Figures

Left shoulder magnetic resonance imaging showing the lesions. (A) Axial plane: Bankart lesion. (B) Sagittal plane: Hill-Sachs lesion. (BL, Bankart lesion; HH, Humeral head; HSL, Hill-Sachs lesion.)

Patient in the beach-chair position; no traction used.
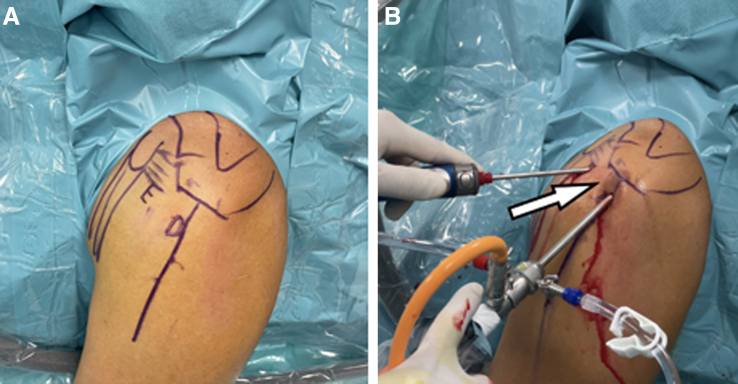
Arthroscopic portals, left shoulder. Viewing portal D. Initial working portal E.

Beach-chair position, left shoulder. View portal D. We identify the coracoacromial ligament (CAL), which will be our superior landmark (A) to remove the rotator interval (RI). We recommend following the coracoacromial ligament from lateral until its insertion in the glenoid process and start opening the rotator interval from this reference to anterior (B). (CAL, coracoacromial ligament; RI, rotator interval; S, supraspinous.)

Beach-chair position, left shoulder. View portal D. For the opening of the rotator interval, we remove the coracohumeral ligament and the superior glenohumeral ligament.

Beach-chair position, left shoulder. View portal D. For the opening of the rotator interval, we remove the coracohumeral ligament and the superior glenohumeral ligament. As we go deeper, care should be taken not to injure the long head of the biceps (LHB), and we should take advantage of this moment to explore the biceps tendon for any pathology that may require treatment.

Beach-chair position, left shoulder. View portal D. We should clean the entire rotator interval and expose the base of the coracoid to avoid postoperative pain and stiffness. We must expose the conjoint tendon and dissect the clavipectoralis fascia to facilitate work on the anterior shoulder. (C, coracoid basis; CT, conjoint tendon; S, supraspinous.)
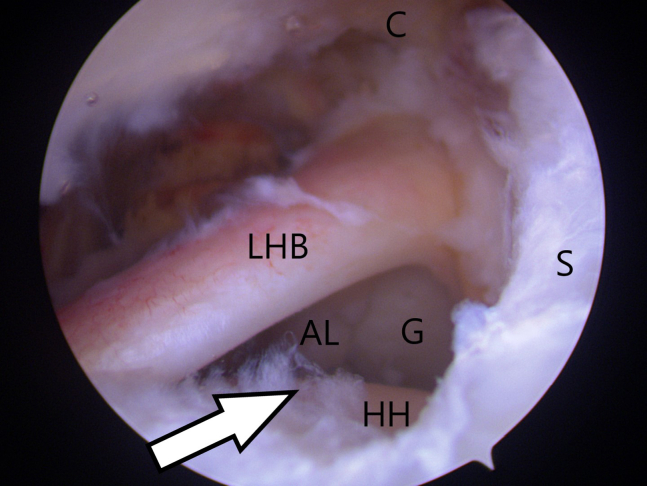
Beach-chair position, left shoulder. View portal D. We move to the intra-articular space with the camera between the long head of the biceps and supraspinatus. Once we have opened the rotator interval, we must perform an exhaustive diagnostic arthroscopy to rule out other articular injuries. (AL, anterior labrum; G, glenoid; HH, humeral head; LHB, long head of the biceps; S, supraspinous.)

Beach-chair position, left shoulder. View portal D. With the arm in retropulsion position, we expose the posterior labrum (A). We perform a posteroinferior percutaneous portal, and without using cannulas, we place an Iconix 1.4 anchor (Stryker) at 7 o'clock (B). A lasso-mattress type suture is performed with a direct suture passer. To do this, we pass one of the threads with a loop lasso and the other one with a direct pass. (G, glenoid; HH, humeral head; PC, posterior capsule; PL, posterior labrum.)

Beach-chair position, left shoulder. View portal D. To treat the Hill-Sachs lesion, an Iconix 2.3 anchor (Stryker) is prepared for remplissage. We pass the 4 threads through the tissue but will not tie the knots until the end of the surgery. The implant is placed in the part closest to the cartilage of the Hill-Sachs defect. The reason for placing the anchor at this time is because if it is placed after repairing the anterior labrum, it could damage the repair. (G, glenoid; HH, humeral head; HSL, Hill-Sachs lesion; PL, posterior labrum.)

Beach-chair position, left shoulder. View portal D. We perform an anteroinferior percutaneous portal (A), just lateral to the conjoint tendon, to have direct access to the anteroinferior glenoid area. This portal allows the anteroinferior anchor to be placed toward the center of the glenoid, where there is usually more bone stock. The detachment of the anterior labrum is performed with a periostotome to lift it to the underside of the glenoid (B). After checking that the anterior labrum can be mobilized and reduced to its anatomic area, the anteroinferior labrum is repaired with an Iconix 1.4 anchor (Stryker) at 5 o'clock. (AL, anterior labrum; G, glenoid; HH, humeral head.)
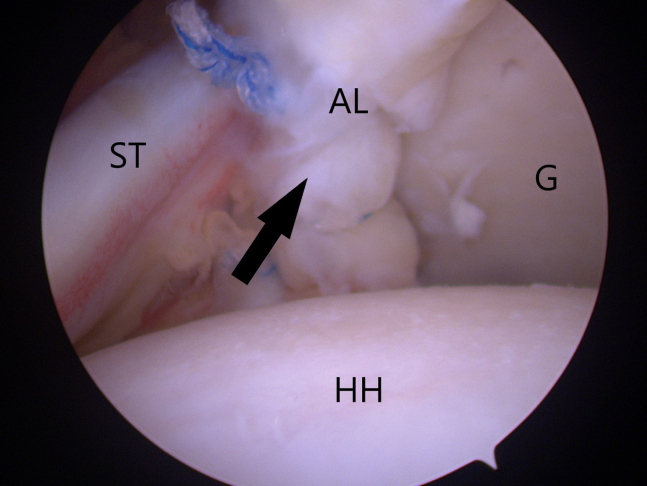
Beach-chair position, left shoulder. View portal D. To repair the anterior labrum, we repeat the same process as for the posterior labrum with a lasso-mattress suture. In total, for the entire anterior labrum, we use 2 to 3 anchors, depending on the tear type. In this step, we must be careful not to place too many implants and avoid placing them too high, as this can cause stiffness in the biceps tendon. (AL, anterior labrum; G, glenoid; HH, humeral head; ST, subscapularis tendon.)

Beach-chair position, left shoulder. View portal D. In the case of anteroinferior instability, the order of knotting is as follows: anteroinferior plication (1), posteroinferior plication (2), anterior plication (3) (from lower to upper), and remplissage (4) as these are lasso-mattress sutures. The post should always be the longest of the threads, as this is the one that has not passed through the loop.
References
LinkOut - more resources
Full Text Sources
