

Short-term efficacy and safety of early medical abortion in Japan: A multicenter prospective study
- PMID: 37013166
- PMCID: PMC10066193
- DOI: 10.1002/rmb2.12512
Short-term efficacy and safety of early medical abortion in Japan: A multicenter prospective study
Abstract
Purpose: To evaluate the short-term efficacy and safety of a combined mifepristone-misoprostol regimen in individuals seeking medical abortion at up to 63 days of gestational age.
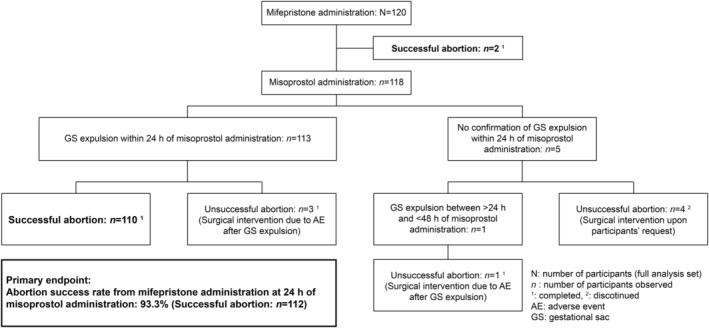
Methods: This open-label, multicenter, prospective study evaluated the short-term efficacy and safety of medical abortion, with the primary outcome being the abortion success rate 24 h after misoprostol administration. The participants received 200 mg of mifepristone orally and 800 μg of misoprostol buccally in the hospital/clinic 36-48 h later. Bleeding and lower abdominal pain, which are the main symptoms associated with medical abortion, were recorded.
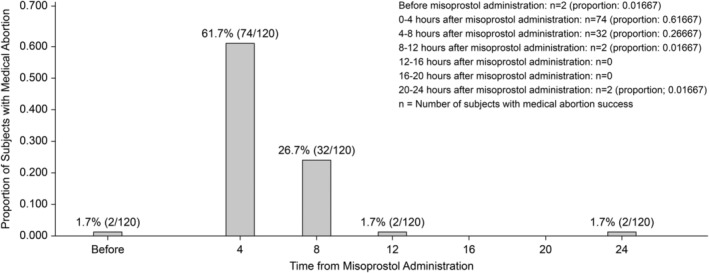
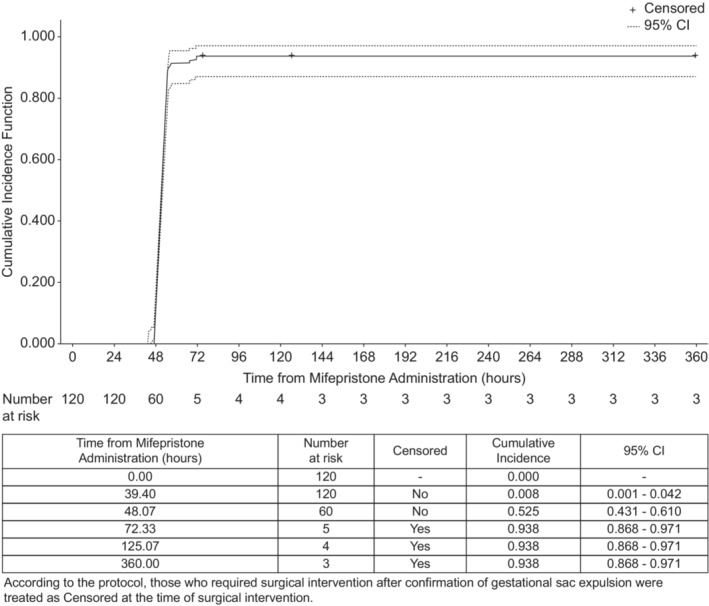
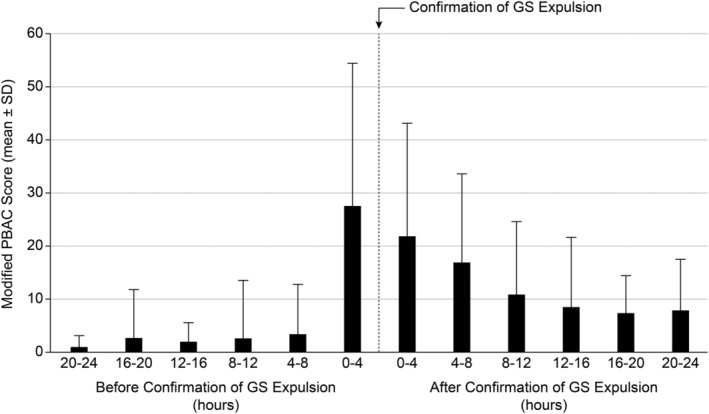
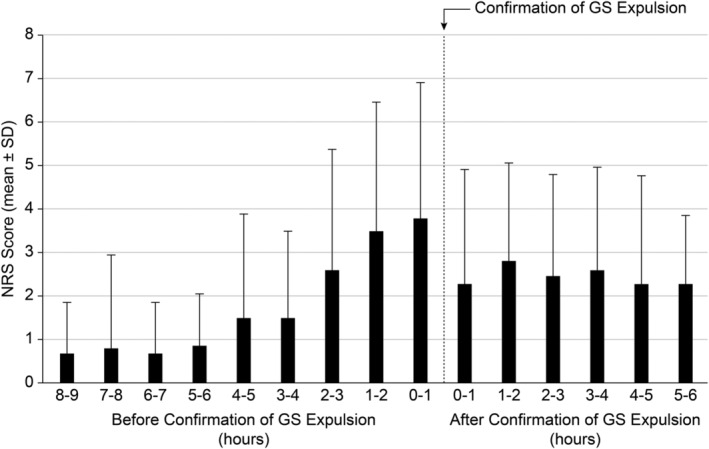
Results: The abortion success rate was 93.3% (95% confidence interval [CI]: 87.3-97.1%) within 24 h of misoprostol administration, 63.3% (95% CI: 54.05-71.94%) within 4 h, and 90.0% (95% CI: 83.18-94.73%) within 8 h. The median time from misoprostol administration to a successful abortion was 3.93 h. Bleeding was most commonly observed 0-4 h prior to the confirmation of gestational sac (GS) expulsion. The most intense lower abdominal pain occurred 0-1 h before the confirmation of GS expulsion.
Conclusion: The combined regimen of mifepristone and buccal misoprostol for medical abortion showed short-term efficacy and a favorable safety profile.
Keywords: Japan; abortion; combination therapy; mifepristone; misoprostol.
© 2023 The Authors. Reproductive Medicine and Biology published by John Wiley & Sons Australia, Ltd on behalf of Japan Society for Reproductive Medicine.
Conflict of interest statement
The authors declare no Conflict of Interests for this article.
Figures
References
-
- World Health Organization . WHO Model List of Essential Medicines (20th List) [Internet]. Geneva: World Health Organization; 2017. (Amended August 2017) [cited 2023 February 1]. https://www.who.int/publications/i/item/eml‐20
-
- Bygdeman M, Swahn ML. Progesterone receptor blockage. Effect on uterine contractility and early pregnancy. Contraception. 1985;32:45–51. - PubMed
-
- Swahn ML, Bygdeman M. The effect of the antiprogestin RU 486 on uterine contractility and sensitivity to prostaglandin and oxytocin. Br J Obstet Gynaecol. 1988;95:126–34. - PubMed
-
- Blum J, Winikoff B, Gemzell‐Danielsson K, Ho PC, Schiavon R, Weeks A. Treatment of incomplete abortion and miscarriage with misoprostol. Int J Gynaecol Obstet. 2007;99(Suppl 2):S186–9. - PubMed
-
- World Health Organization . Medical Management of Abortion [internet]. Geneva: World Health Organization; 2018. [cited 2023 February 1]. https://apps.who.int/iris/bitstream/handle/10665/278968/9789241550406‐en...
LinkOut - more resources
Full Text Sources