

A novel transcriptional signature identifies T-cell infiltration in high-risk paediatric cancer
- PMID: 37013636
- PMCID: PMC10071693
- DOI: 10.1186/s13073-023-01170-x
A novel transcriptional signature identifies T-cell infiltration in high-risk paediatric cancer
Abstract
Background: Molecular profiling of the tumour immune microenvironment (TIME) has enabled the rational choice of immunotherapies in some adult cancers. In contrast, the TIME of paediatric cancers is relatively unexplored. We speculated that a more refined appreciation of the TIME in childhood cancers, rather than a reliance on commonly used biomarkers such as tumour mutation burden (TMB), neoantigen load and PD-L1 expression, is an essential prerequisite for improved immunotherapies in childhood solid cancers.
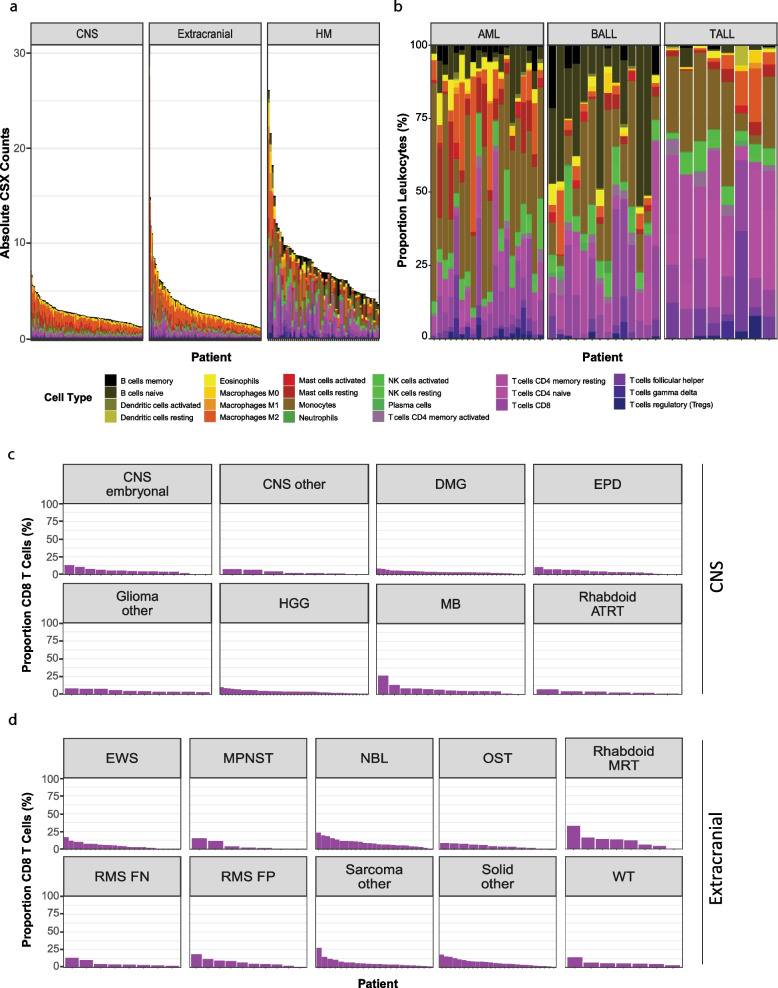
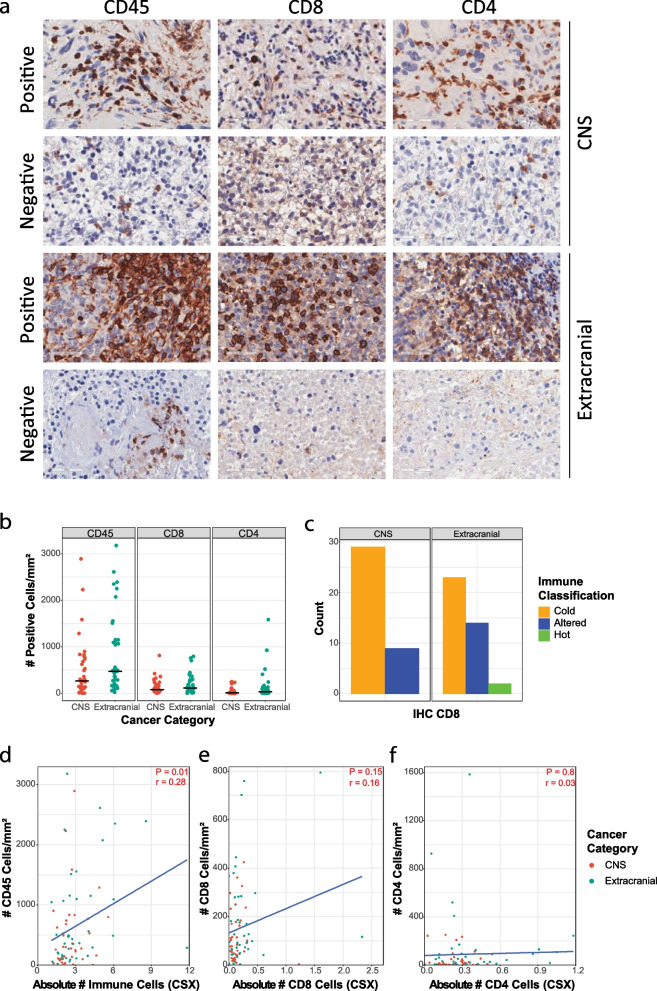
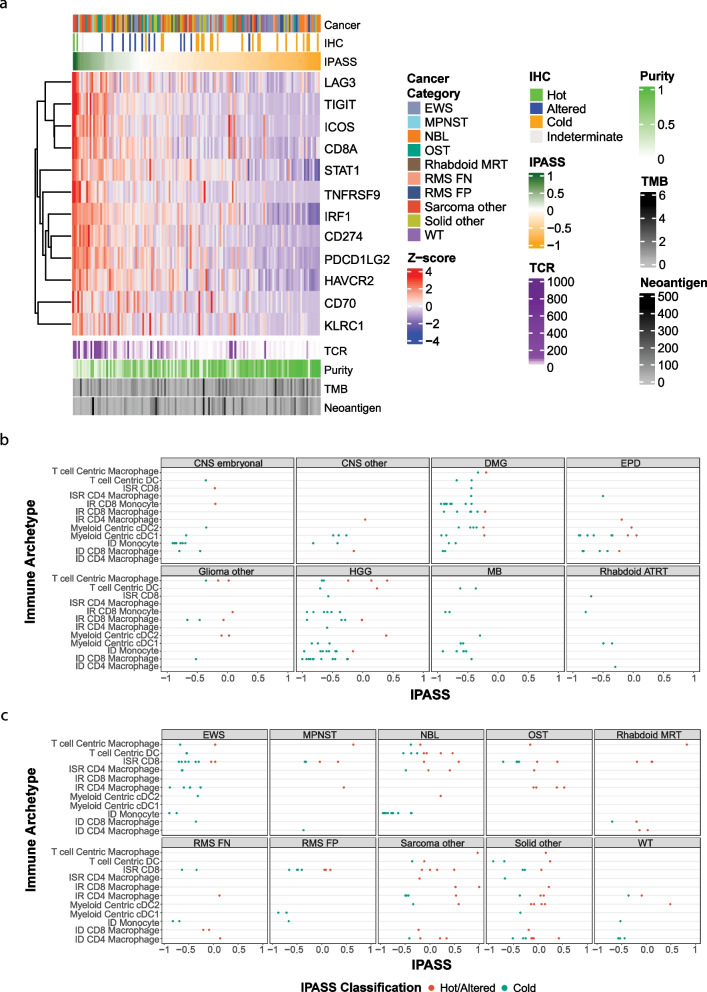
Methods: We combined immunohistochemistry (IHC) with RNA sequencing and whole-genome sequencing across a diverse spectrum of high-risk paediatric cancers to develop an alternative, expression-based signature associated with CD8+ T-cell infiltration of the TIME. Furthermore, we explored transcriptional features of immune archetypes and T-cell receptor sequencing diversity, assessed the relationship between CD8+ and CD4+ abundance by IHC and deconvolution predictions and assessed the common adult biomarkers such as neoantigen load and TMB.
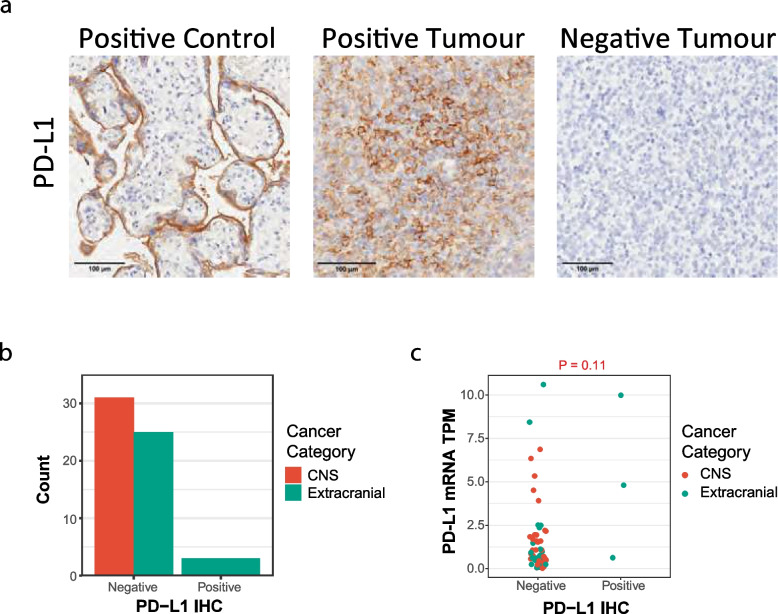
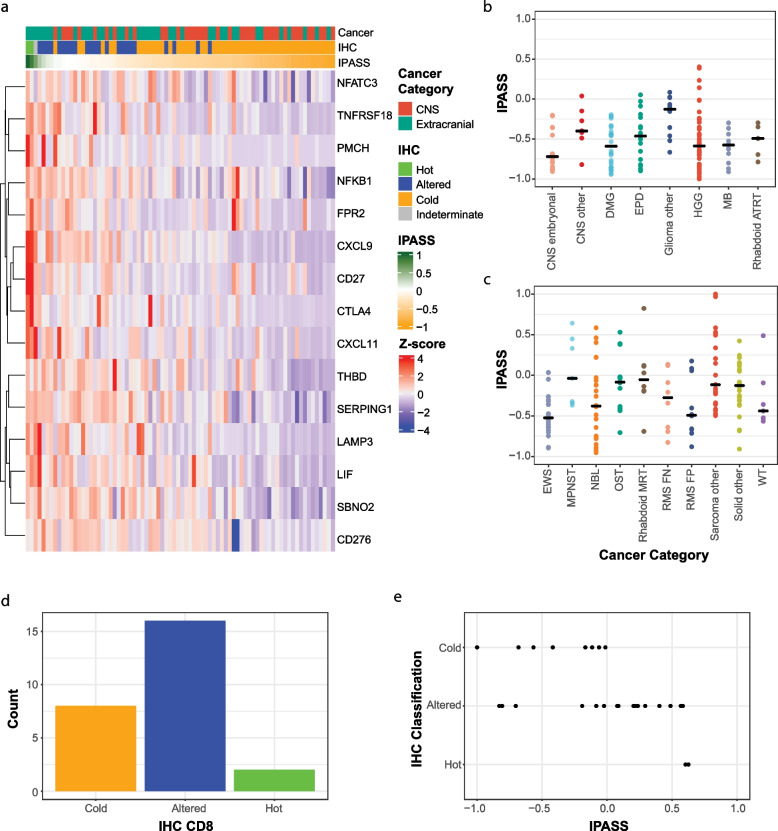
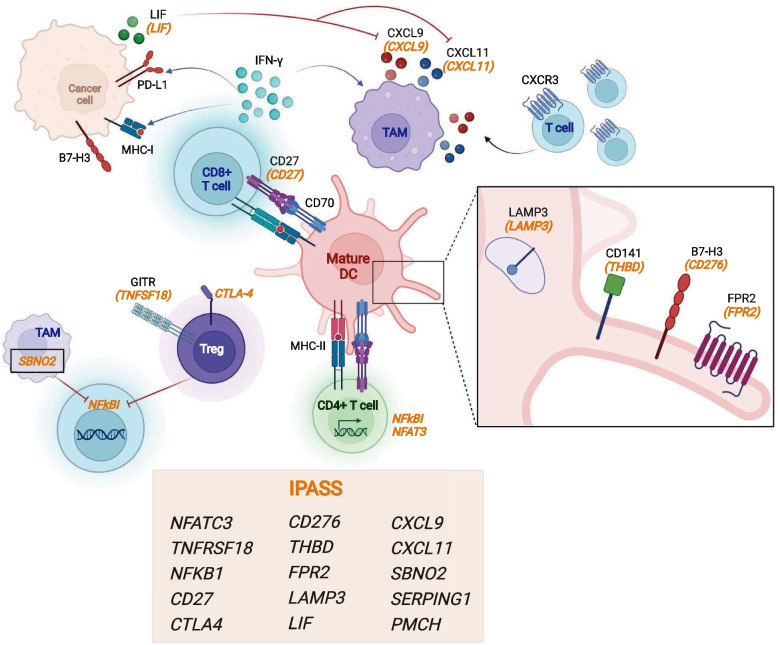
Results: A novel 15-gene immune signature, Immune Paediatric Signature Score (IPASS), was identified. Using this signature, we estimate up to 31% of high-risk cancers harbour infiltrating T-cells. In addition, we showed that PD-L1 protein expression is poorly correlated with PD-L1 RNA expression and TMB and neoantigen load are not predictive of T-cell infiltration in paediatrics. Furthermore, deconvolution algorithms are only weakly correlated with IHC measurements of T-cells.
Conclusions: Our data provides new insights into the variable immune-suppressive mechanisms dampening responses in paediatric solid cancers. Effective immune-based interventions in high-risk paediatric cancer will require individualised analysis of the TIME.
Keywords: Biomarkers; Paediatric cancer; T-cell infiltration; Transcriptome signature; Tumour immune microenvironment.
© 2023. The Author(s).
Conflict of interest statement
P.G.E receives an annual payment related to the Walter and Eliza Hall Institute distribution of royalties scheme. P.G.E. consults for Illumina. P.J.N. receives research funding from BMS, Roche Genentech, Allergan, Compugen, Merck Sharpe Dohme and Crispr therapeutics. J.R.H. declares honorarium or Bayer and Alexion Pharmaceuticals; Boxer Capital unrelated to this work. The remaining authors declare that they have no competing interests.
Figures
References
-
- van Tilburg CM, Pfaff E, Pajtler KW, Langenberg KPS, Fiesel P, Jones BC, et al. The Pediatric Precision Oncology INFORM Registry: clinical outcome and benefit for patients with very high-evidence targets. Cancer Discov. 2021;11(11):2764–2779. doi: 10.1158/2159-8290.CD-21-0094. - DOI - PMC - PubMed
-
- Expanding the reach of anti-PD-1 therapy. Cancer Discov. 2015;5(7):684–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
