

Platform combining statistical modeling and patient-derived organoids to facilitate personalized treatment of colorectal carcinoma
- PMID: 37013646
- PMCID: PMC10069117
- DOI: 10.1186/s13046-023-02650-z
Platform combining statistical modeling and patient-derived organoids to facilitate personalized treatment of colorectal carcinoma
Abstract
Background: We propose a new approach for designing personalized treatment for colorectal cancer (CRC) patients, by combining ex vivo organoid efficacy testing with mathematical modeling of the results.
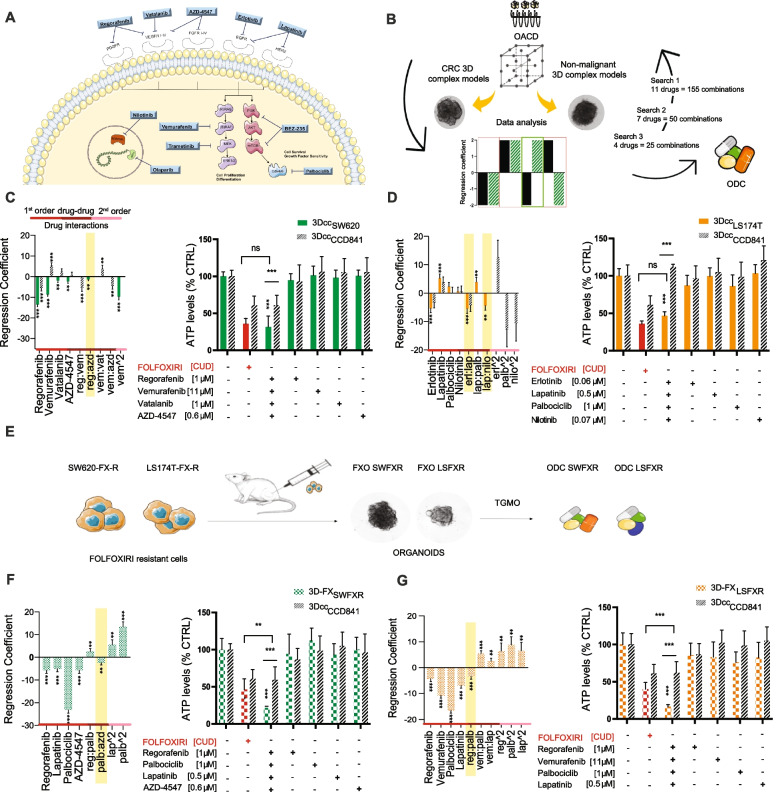
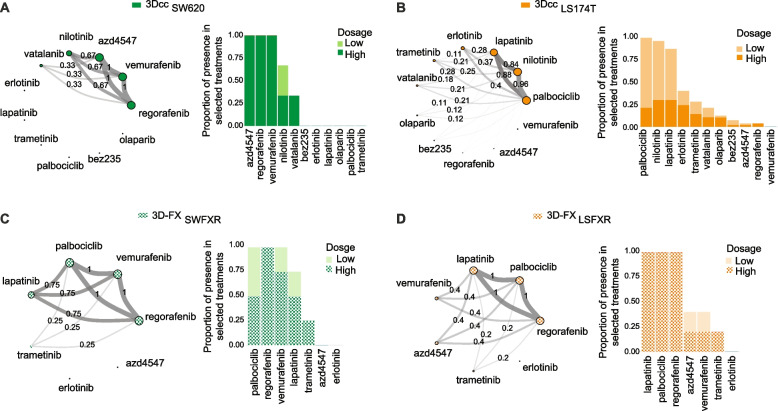
Methods: The validated phenotypic approach called Therapeutically Guided Multidrug Optimization (TGMO) was used to identify four low-dose synergistic optimized drug combinations (ODC) in 3D human CRC models of cells that are either sensitive or resistant to first-line CRC chemotherapy (FOLFOXIRI). Our findings were obtained using second order linear regression and adaptive lasso.
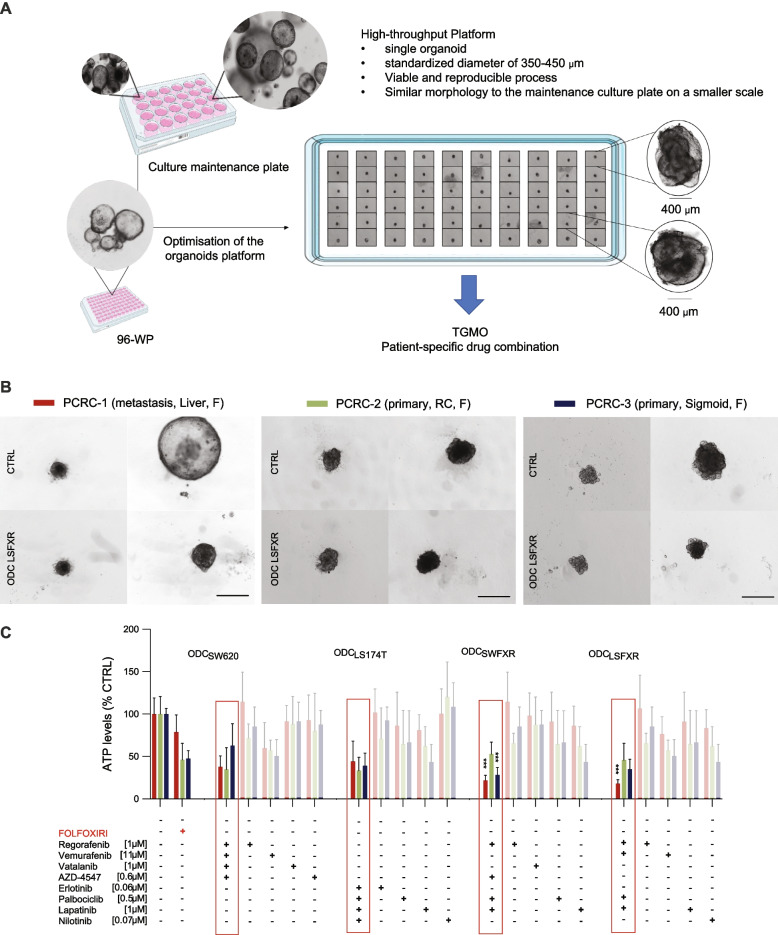
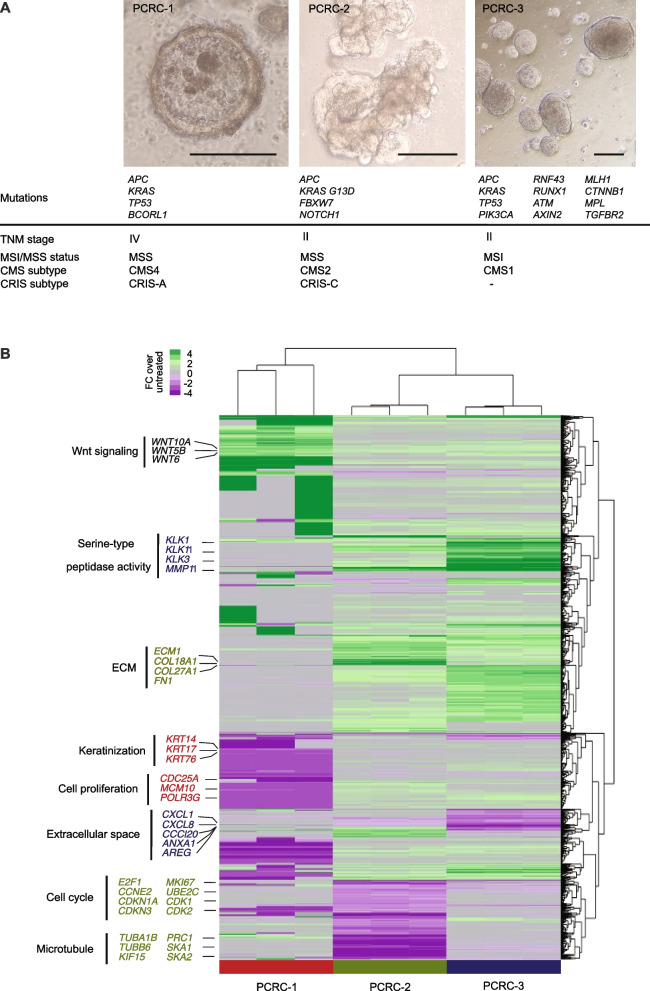
Results: The activity of all ODCs was validated on patient-derived organoids (PDO) from cases with either primary or metastatic CRC. The CRC material was molecularly characterized using whole-exome sequencing and RNAseq. In PDO from patients with liver metastases (stage IV) identified as CMS4/CRIS-A, our ODCs consisting of regorafenib [1 mM], vemurafenib [11 mM], palbociclib [1 mM] and lapatinib [0.5 mM] inhibited cell viability up to 88%, which significantly outperforms FOLFOXIRI administered at clinical doses. Furthermore, we identified patient-specific TGMO-based ODCs that outperform the efficacy of the current chemotherapy standard of care, FOLFOXIRI.
Conclusions: Our approach allows the optimization of patient-tailored synergistic multi-drug combinations within a clinically relevant timeframe.
Keywords: Drug resistance; Drug-drug interaction; Multidrug combination; Organoid; Phenotypic screen; Synergy; Targeted RNAseq.
© 2023. The Author(s).
Conflict of interest statement
P.N.-S. is inventor of a patent of drug combination optimization methods. The other authors declare no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
