

Review
doi: 10.1152/physiol.00004.2023.
Epub 2023 Apr 4.
Inflammatory Mechanisms in Heart Failure with Preserved Ejection Fraction
Affiliations
- PMID: 37013947
- PMCID: PMC10396273
- DOI: 10.1152/physiol.00004.2023
Item in Clipboard
Review
Inflammatory Mechanisms in Heart Failure with Preserved Ejection Fraction
Physiology (Bethesda).
.
Abstract
Heart failure with preserved ejection fraction (HFpEF) is now the most common form of heart failure and a significant public health concern for which limited effective therapies exist. Inflammation triggered by comorbidity burden is a critical element of HFpEF pathophysiology. Here, we discuss evidence for comorbidity-driven systemic and myocardial inflammation and the mechanistic role of inflammation in pathological myocardial remodeling in HFpEF.
Keywords: heart failure; inflammation; meta-inflammation; myocardial remodeling.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
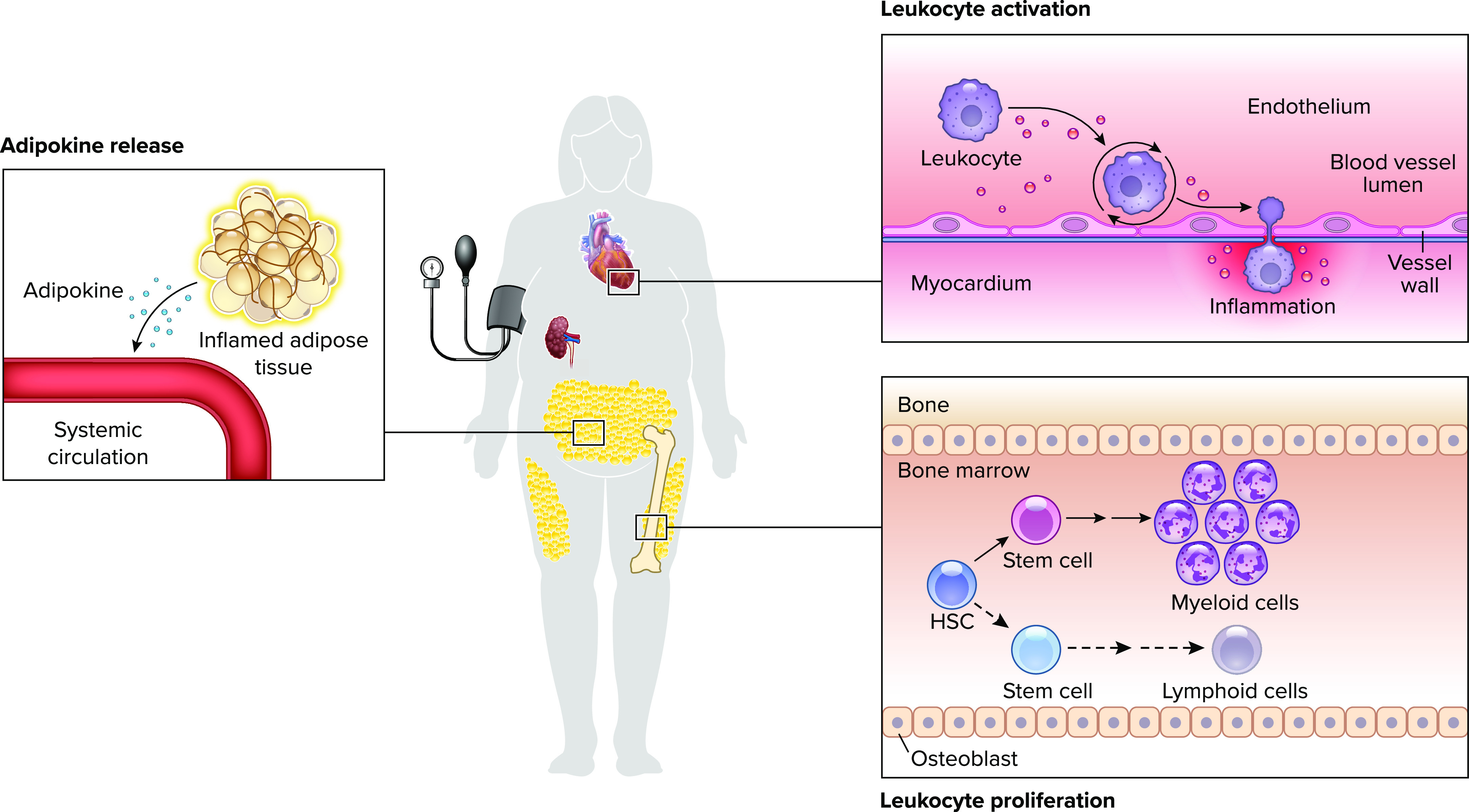
Heart failure with preserved ejection fraction-associated comorbidities increase circulating and activated, myocardium-infiltrating leukocytes Adipose tissue, in turn, contributes to circulating inflammatory signals. The resulting systemic and myocardial inflammation is characteristic of heart failure with preserved ejection fraction (HFpEF). HSC, hematopoietic stem cell.
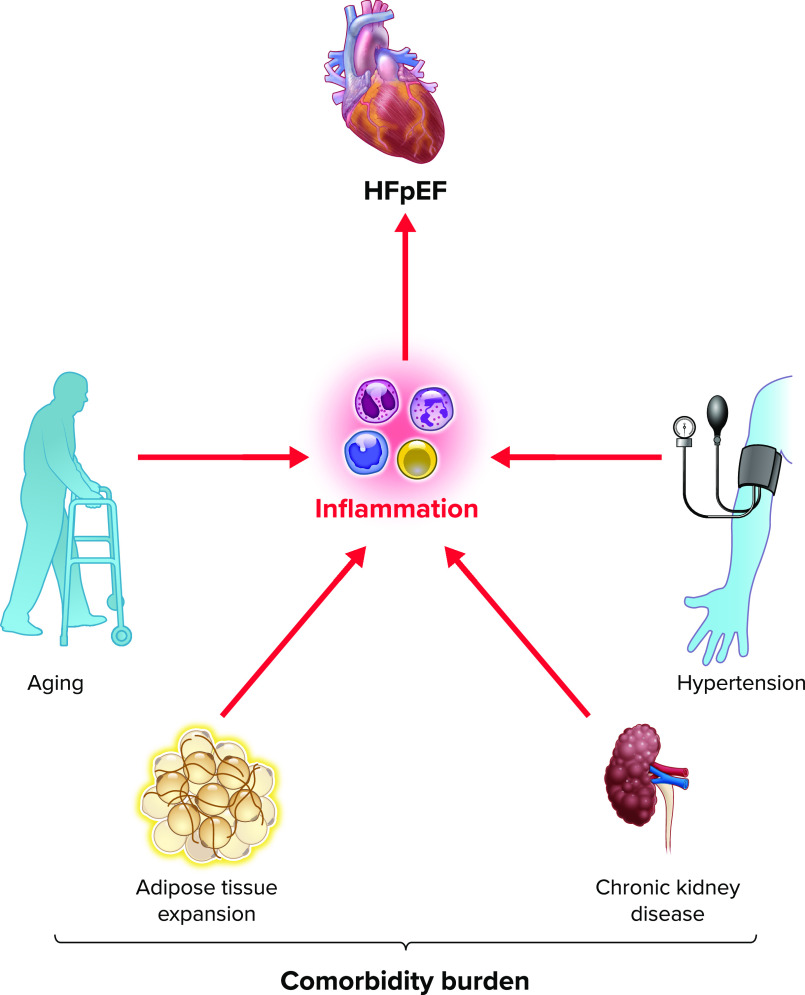
Depicted are common comorbidities associated with HFpEF Each comorbidity is associated with, and drives, low-grade, systemic inflammation.
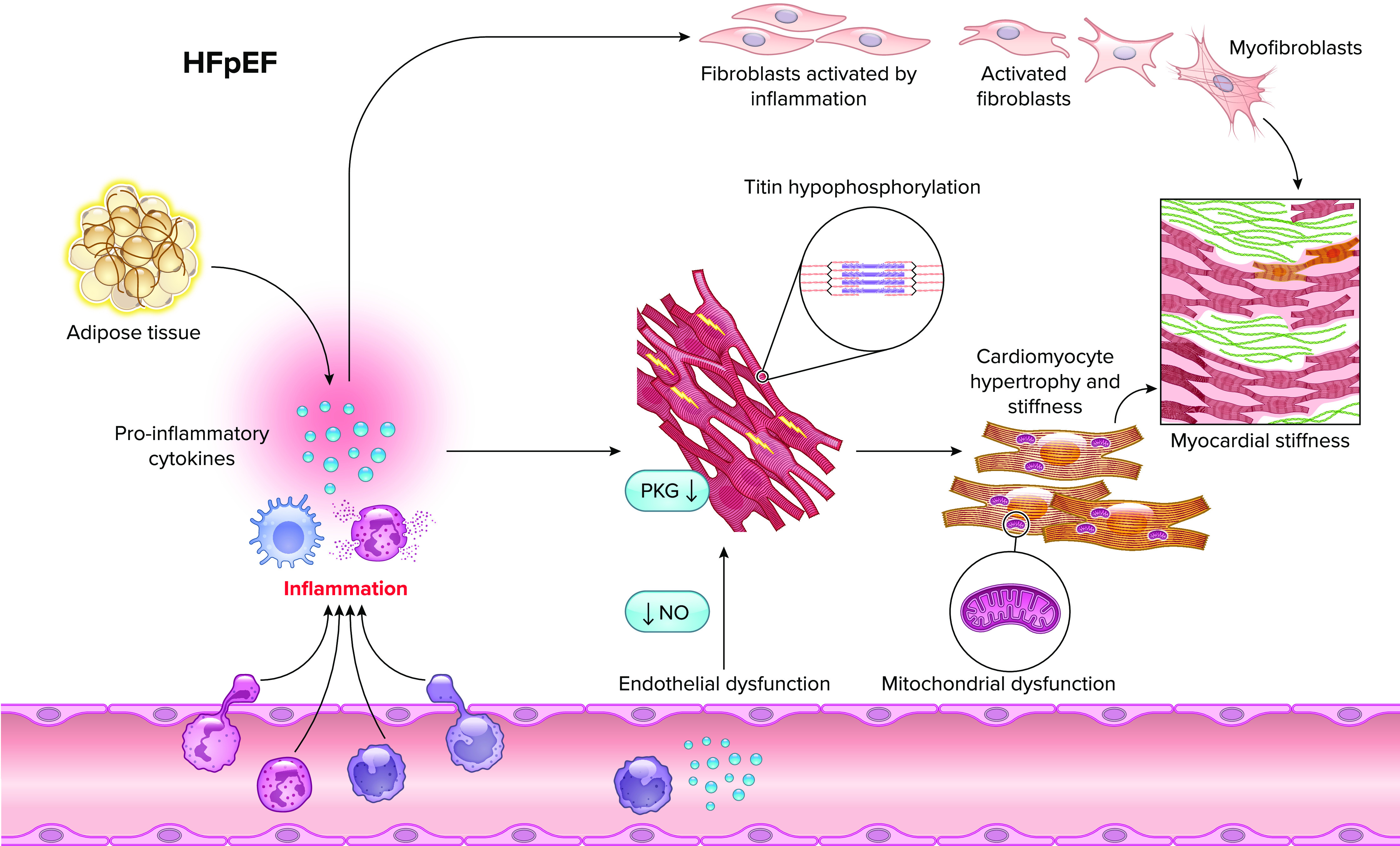
Inflammation underpins pathological cardiomyocyte and fibroblast alterations that contribute to myocardial stiffness in HFpEF NO, nitric oxide.
References
-
- Schiattarella GG, Alcaide P, Condorelli G, Gillette TG, Heymans S, Jones EA, Kallikourdis M, Lichtman A, Marelli-Berg F, Shah S, Thorp EB, Hill JA. Immunometabolic mechanisms of heart failure with preserved ejection fraction. Nat Cardiovasc Res 1: 211–222, 2022. doi:10.1038/s44161-022-00032-w. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical