

The impact of varying the number and selection of conditions on estimated multimorbidity prevalence: A cross-sectional study using a large, primary care population dataset
- PMID: 37014910
- PMCID: PMC10072475
- DOI: 10.1371/journal.pmed.1004208
The impact of varying the number and selection of conditions on estimated multimorbidity prevalence: A cross-sectional study using a large, primary care population dataset
Abstract
Background: Multimorbidity prevalence rates vary considerably depending on the conditions considered in the morbidity count, but there is no standardised approach to the number or selection of conditions to include.
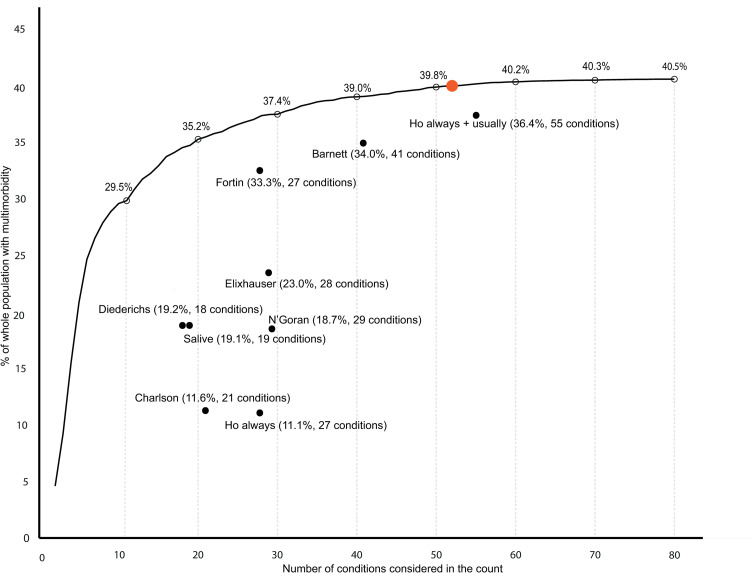
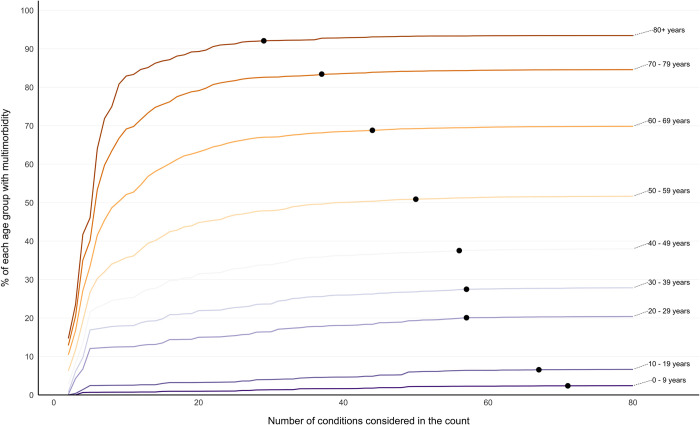
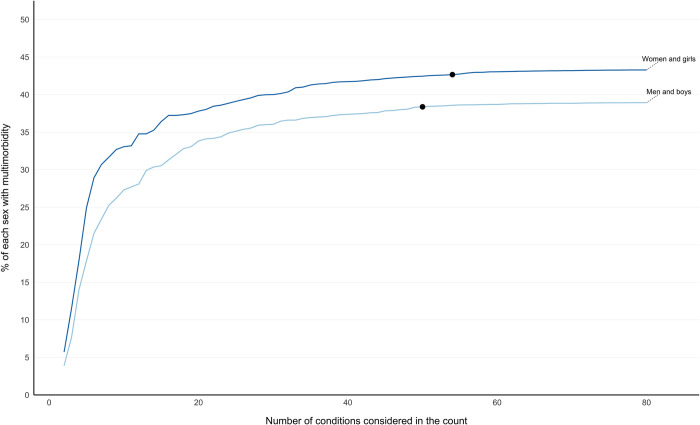
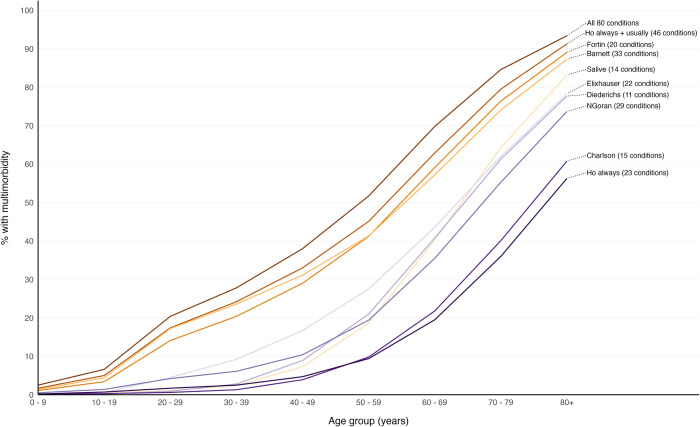
Methods and findings: We conducted a cross-sectional study using English primary care data for 1,168,260 participants who were all people alive and permanently registered with 149 included general practices. Outcome measures of the study were prevalence estimates of multimorbidity (defined as ≥2 conditions) when varying the number and selection of conditions considered for 80 conditions. Included conditions featured in ≥1 of the 9 published lists of conditions examined in the study and/or phenotyping algorithms in the Health Data Research UK (HDR-UK) Phenotype Library. First, multimorbidity prevalence was calculated when considering the individually most common 2 conditions, 3 conditions, etc., up to 80 conditions. Second, prevalence was calculated using 9 condition-lists from published studies. Analyses were stratified by dependent variables age, socioeconomic position, and sex. Prevalence when only the 2 commonest conditions were considered was 4.6% (95% CI [4.6, 4.6] p < 0.001), rising to 29.5% (95% CI [29.5, 29.6] p < 0.001) considering the 10 commonest, 35.2% (95% CI [35.1, 35.3] p < 0.001) considering the 20 commonest, and 40.5% (95% CI [40.4, 40.6] p < 0.001) when considering all 80 conditions. The threshold number of conditions at which multimorbidity prevalence was >99% of that measured when considering all 80 conditions was 52 for the whole population but was lower in older people (29 in >80 years) and higher in younger people (71 in 0- to 9-year-olds). Nine published condition-lists were examined; these were either recommended for measuring multimorbidity, used in previous highly cited studies of multimorbidity prevalence, or widely applied measures of "comorbidity." Multimorbidity prevalence using these lists varied from 11.1% to 36.4%. A limitation of the study is that conditions were not always replicated using the same ascertainment rules as previous studies to improve comparability across condition-lists, but this highlights further variability in prevalence estimates across studies.
Conclusions: In this study, we observed that varying the number and selection of conditions results in very large differences in multimorbidity prevalence, and different numbers of conditions are needed to reach ceiling rates of multimorbidity prevalence in certain groups of people. These findings imply that there is a need for a standardised approach to defining multimorbidity, and to facilitate this, researchers can use existing condition-lists associated with highest multimorbidity prevalence.
Copyright: © 2023 MacRae et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Multimorbidity: a priority for global health research. The Academy of Medical Sciences. Available from: https://acmedsci.ac.uk/policy/policy-projects/multimorbidity [accessed 2022 Apr 18].
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
