

Schistosomiasis screening in non-endemic countries from a cost perspective: Knowledge gaps and research priorities. The case of African long-term residents in a Metropolitan Area, Spain
- PMID: 37014919
- PMCID: PMC10104311
- DOI: 10.1371/journal.pntd.0011221
Schistosomiasis screening in non-endemic countries from a cost perspective: Knowledge gaps and research priorities. The case of African long-term residents in a Metropolitan Area, Spain
Abstract
Background: Imported schistosomiasis is an emerging issue in European countries as a result of growing global migration from schistosomiasis-endemic countries, mainly in sub-Saharan Africa. Undetected infection may lead to serious long-term complications with an associated high cost for public healthcare systems especially among long-term migrants.
Objective: To evaluate from a health economics perspective the introduction of schistosomiasis screening programs in non-endemic countries with high prevalence of long-term migrants.
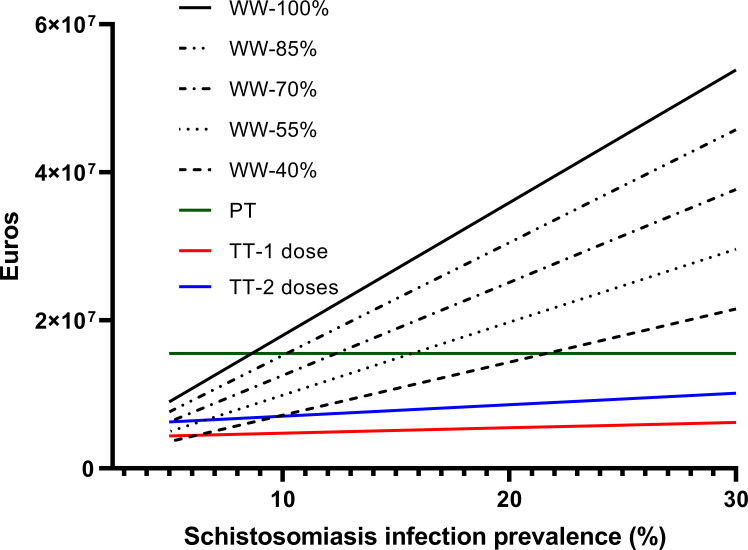
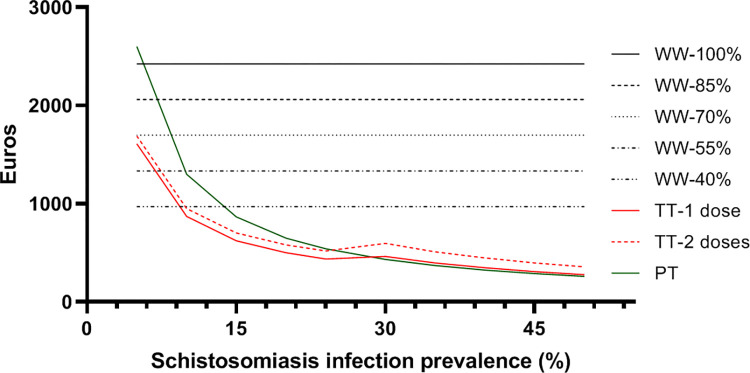
Methodology: We calculated the costs associated with three approaches-presumptive treatment, test-and-treat and watchful waiting-under different scenarios of prevalence, treatment efficacy and the cost of care resulting from long-term morbidity. Costs were estimated for our study area, in which there are reported to reside 74,000 individuals who have been exposed to the infection. Additionally, we methodically reviewed the potential factors that could affect the cost/benefit ratio of a schistosomiasis screening program and need therefore to be ascertained.
Results: Assuming a 24% prevalence of schistosomiasis in the exposed population and 100% treatment efficacy, the estimated associated cost per infected person of a watchful waiting strategy would be €2,424, that of a presumptive treatment strategy would be €970 and that of a test-and-treat strategy would be €360. The difference in averted costs between test-and-treat and watchful waiting strategies ranges from nearly €60 million in scenarios of high prevalence and treatment efficacy, to a neutral costs ratio when these parameters are halved. However, there are important gaps in our understanding of issues such as the efficacy of treatment in infected long-term residents, the natural history of schistosomiasis in long-term migrants and the feasibility of screening programs.
Conclusion: Our results support the roll-out of a schistosomiasis screening program based on a test-and-treat strategy from a health economics perspective under the most likely projected scenarios, but important knowledge gaps should be addressed for a more accurate estimations among long-term migrants.
Copyright: © 2023 Roure et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Global Burden of Disease 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1859–922. doi: 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- World Health Organization. Schistosomiasis and soil-transmitted helminthiases: numbers of people treated in 2018. Wkly Epidemiol Rec 2018; 94: 601–12.
MeSH terms
LinkOut - more resources
Full Text Sources
