

Nationwide Trends and Determinants of Germline BRCA1/2 Testing in Patients With Breast and Ovarian Cancer
- PMID: 37015340
- PMCID: PMC10256435
- DOI: 10.6004/jnccn.2022.7257
Nationwide Trends and Determinants of Germline BRCA1/2 Testing in Patients With Breast and Ovarian Cancer
Abstract
Background: Germline genetic testing (GT) for BRCA1/2 is instrumental in identifying patients with breast and ovarian cancers who are eligible for PARP inhibitors (PARPi). Little is known about recent trends and determinants of GT since PARPi were approved for these patients.
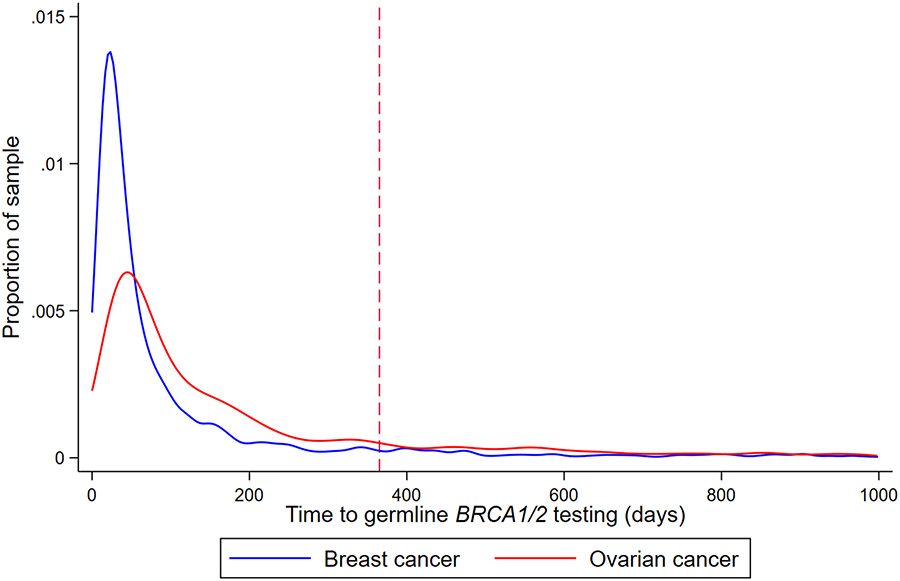
Patients and methods: We performed a retrospective cohort study of patients in a nationwide electronic health record (EHR)-derived oncology-specific database with the following GT eligibility criteria: breast cancer diagnosed at age ≤45 years, triple-negative breast cancer diagnosed at age ≤60 years, male breast cancer, or ovarian cancer. GT within 1 year of diagnosis was assessed and stratified by tumor type. Multivariable log-binomial regressions estimated adjusted relative risks (RRs) of GT by patient and tumor characteristics.
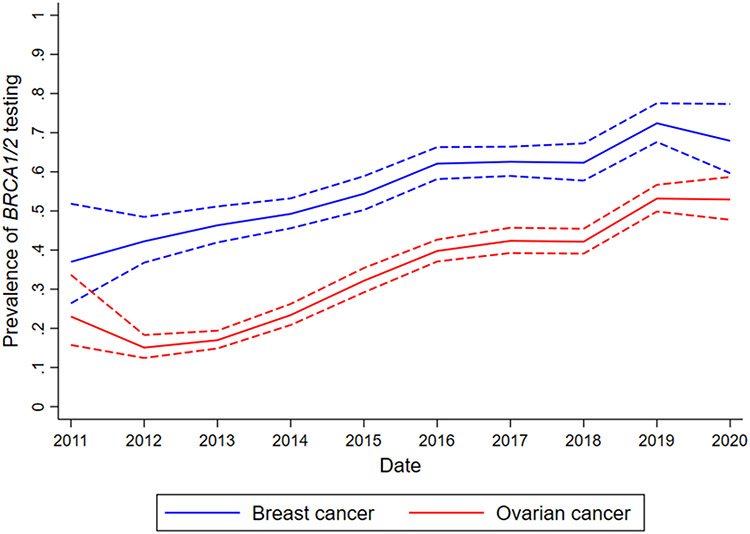
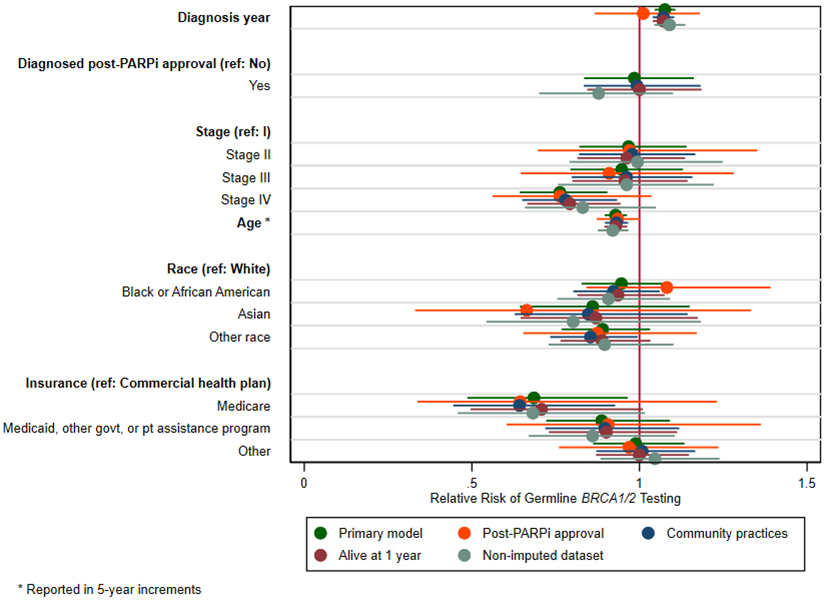
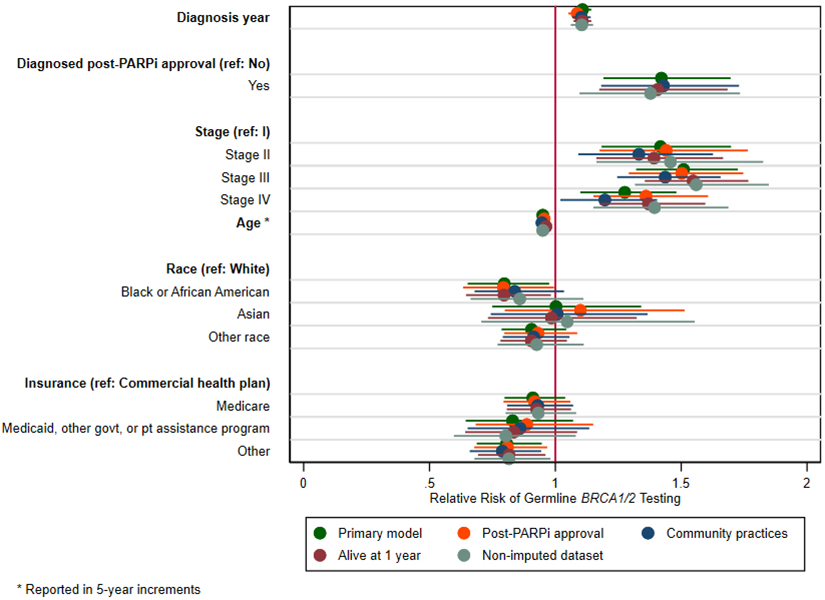
Results: Among 2,982 eligible patients with breast cancer, 56.4% underwent GT between January 2011 and March 2020, with a significant increase in GT over time (RR, 1.08; 95% CI, 1.05-1.11, for each year), independent of when PARPi were approved for BRCA1/2-mutated metastatic breast cancer in January 2018. In multivariable analyses, older age (RR, 0.93; 95% CI, 0.90-0.96, for every 5 years) and Medicare coverage (RR, 0.69; 95% CI, 0.49-0.96 vs commercial insurance) were associated with less GT. Among 5,563 eligible patients with ovarian cancer, 35.4% underwent GT between January 2011 and March 2020, with a significant increase in GT over time (RR, 1.11; 95% CI, 1.07-1.14, for each year) that accelerated after approval of PARPi for BRCA1/2-mutated, chemotherapy-refractory ovarian cancer in December 2014 (RR, 1.42; 95% CI, 1.19-1.70). Older age (RR, 0.95; 95% CI, 0.93-0.97, for every 5 years) and Black or African American race (RR, 0.80; 95% CI, 0.65-0.98 vs White race) were associated with less GT.
Conclusions: GT remains underutilized nationwide among patients with breast and ovarian cancers. Although GT has increased over time, significant disparities by age, race, and insurance status persist. Additional work is needed to design, implement, and evaluate strategies to ensure that all eligible patients receive GT.
Keywords: Ovarian cancer; breast cancer; germline genetic testing; guideline adherence.
Figures
Comment in
-
Casting a Wide Net While Building a Safety Net: Addressing Disparities in Genetic Testing for Hereditary Cancer.J Natl Compr Canc Netw. 2023 Apr;21(4):430-432. doi: 10.6004/jnccn.2023.7019. J Natl Compr Canc Netw. 2023. PMID: 37015334 No abstract available.
References
-
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. Jama. 2017;317(23):2402–2416. - PubMed
-
- National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines); 2020. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
