

Pulse Wave Amplitude Drops Index: A Biomarker of Cardiovascular Risk in Obstructive Sleep Apnea
- PMID: 37017487
- PMCID: PMC10273112
- DOI: 10.1164/rccm.202206-1223OC
Pulse Wave Amplitude Drops Index: A Biomarker of Cardiovascular Risk in Obstructive Sleep Apnea
Erratum in
-
Erratum: Pulse Wave Amplitude Drops Index: A Biomarker of Cardiovascular Risk in Obstructive Sleep Apnea.Am J Respir Crit Care Med. 2024 Feb 1;209(3):345. doi: 10.1164/rccm.v209erratum1. Am J Respir Crit Care Med. 2024. PMID: 38299879 Free PMC article. No abstract available.
Abstract
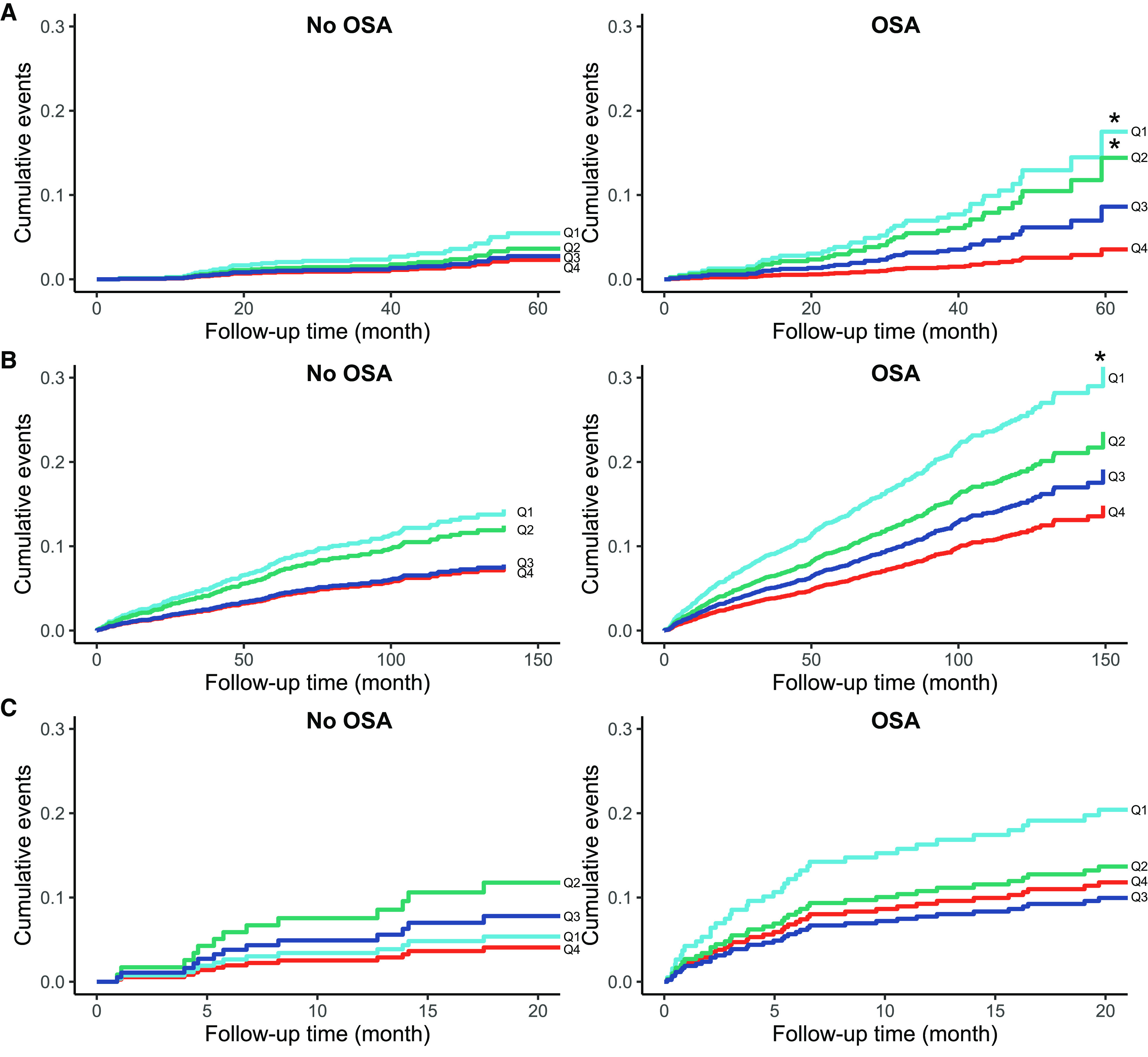
Rationale: It is currently unclear which patients with obstructive sleep apnea (OSA) are at increased cardiovascular risk. Objective: To investigate the value of pulse wave amplitude drops (PWADs), reflecting sympathetic activations and vasoreactivity, as a biomarker of cardiovascular risk in OSA. Methods: PWADs were derived from pulse oximetry-based photoplethysmography signals in three prospective cohorts: HypnoLaus (N = 1,941), the Pays-de-la-Loire Sleep Cohort (PLSC; N = 6,367), and "Impact of Sleep Apnea syndrome in the evolution of Acute Coronary syndrome. Effect of intervention with CPAP" (ISAACC) (N = 692). The PWAD index was the number of PWADs (>30%) per hour during sleep. All participants were divided into subgroups according to the presence or absence of OSA (defined as ⩾15 or more events per hour or <15/h, respectively, on the apnea-hypopnea index) and the median PWAD index. Primary outcome was the incidence of composite cardiovascular events. Measurements and Main Results: Using Cox models adjusted for cardiovascular risk factors (hazard ratio; HR [95% confidence interval]), patients with a low PWAD index and OSA had a higher incidence of cardiovascular events compared with the high-PWAD and OSA group and those without OSA in the HypnoLaus cohort (HR, 2.16 [1.07-4.34], P = 0.031; and 2.35 [1.12-4.93], P = 0.024) and in the PLSC (1.36 [1.13-1.63], P = 0.001; and 1.44 [1.06-1.94], P = 0.019), respectively. In the ISAACC cohort, the low-PWAD and OSA untreated group had a higher cardiovascular event recurrence rate than that of the no-OSA group (2.03 [1.08-3.81], P = 0.028). In the PLSC and HypnoLaus cohorts, every increase of 10 events per hour in the continuous PWAD index was negatively associated with incident cardiovascular events exclusively in patients with OSA (HR, 0.85 [0.73-0.99], P = 0.031; and HR, 0.91 [0.86-0.96], P < 0.001, respectively). This association was not significant in the no-OSA group and the ISAACC cohort. Conclusions: In patients with OSA, a low PWAD index reflecting poor autonomic and vascular reactivity was independently associated with a higher cardiovascular risk.
Keywords: PWAD; cardiovascular risk; pulse oximeter; pulse wave amplitude; sleep apnea.
Figures






Comment in
-
Searching for a Vulnerable Cardiovascular Endotype in Obstructive Sleep Apnea: Is the Humble Pulse Wave a Useful Biomarker?Am J Respir Crit Care Med. 2023 Jun 15;207(12):1553-1555. doi: 10.1164/rccm.202304-0739ED. Am J Respir Crit Care Med. 2023. PMID: 37141108 Free PMC article. No abstract available.
-
Night to night variability of Pulse Wave Amplitude Drops index.Sleep Med. 2024 May;117:60-61. doi: 10.1016/j.sleep.2024.03.019. Epub 2024 Mar 15. Sleep Med. 2024. PMID: 38507978 No abstract available.
References
-
- Pevernagie DA, Gnidovec-Strazisar B, Grote L, Heinzer R, McNicholas WT, Penzel T, et al. On the rise and fall of the apnea-hypopnea index: a historical review and critical appraisal. J Sleep Res . 2020;29:e13066. - PubMed
-
- McEvoy RD, Antic NA, Heeley E, Luo Y, Ou Q, Zhang X, et al. SAVE Investigators and Coordinators CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med . 2016;375:919–931. - PubMed
-
- Peker Y, Glantz H, Eulenburg C, Wegscheider K, Herlitz J, Thunström E. Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease patients with nonsleepy obstructive sleep apnea. The RICCADSA randomized controlled trial. Am J Respir Crit Care Med . 2016;194:613–620. - PubMed
-
- Sánchez-de-la-Torre M, Sánchez-de-la-Torre A, Bertran S, Abad J, Duran-Cantolla J, Cabriada V, et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): a randomised controlled trial. Lancet Respir Med . 2019;8:359–367. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
