

Major Cardiovascular Events After Spontaneous Intracerebral Hemorrhage by Hematoma Location
- PMID: 37017964
- PMCID: PMC10077102
- DOI: 10.1001/jamanetworkopen.2023.5882
Major Cardiovascular Events After Spontaneous Intracerebral Hemorrhage by Hematoma Location
Abstract
Importance: Survivors of spontaneous (ie, nontraumatic and with no known structural cause) intracerebral hemorrhage (ICH) have an increased risk of major cardiovascular events (MACEs), including recurrent ICH, ischemic stroke (IS), and myocardial infarction (MI). Only limited data are available from large, unselected population studies assessing the risk of MACEs according to index hematoma location.
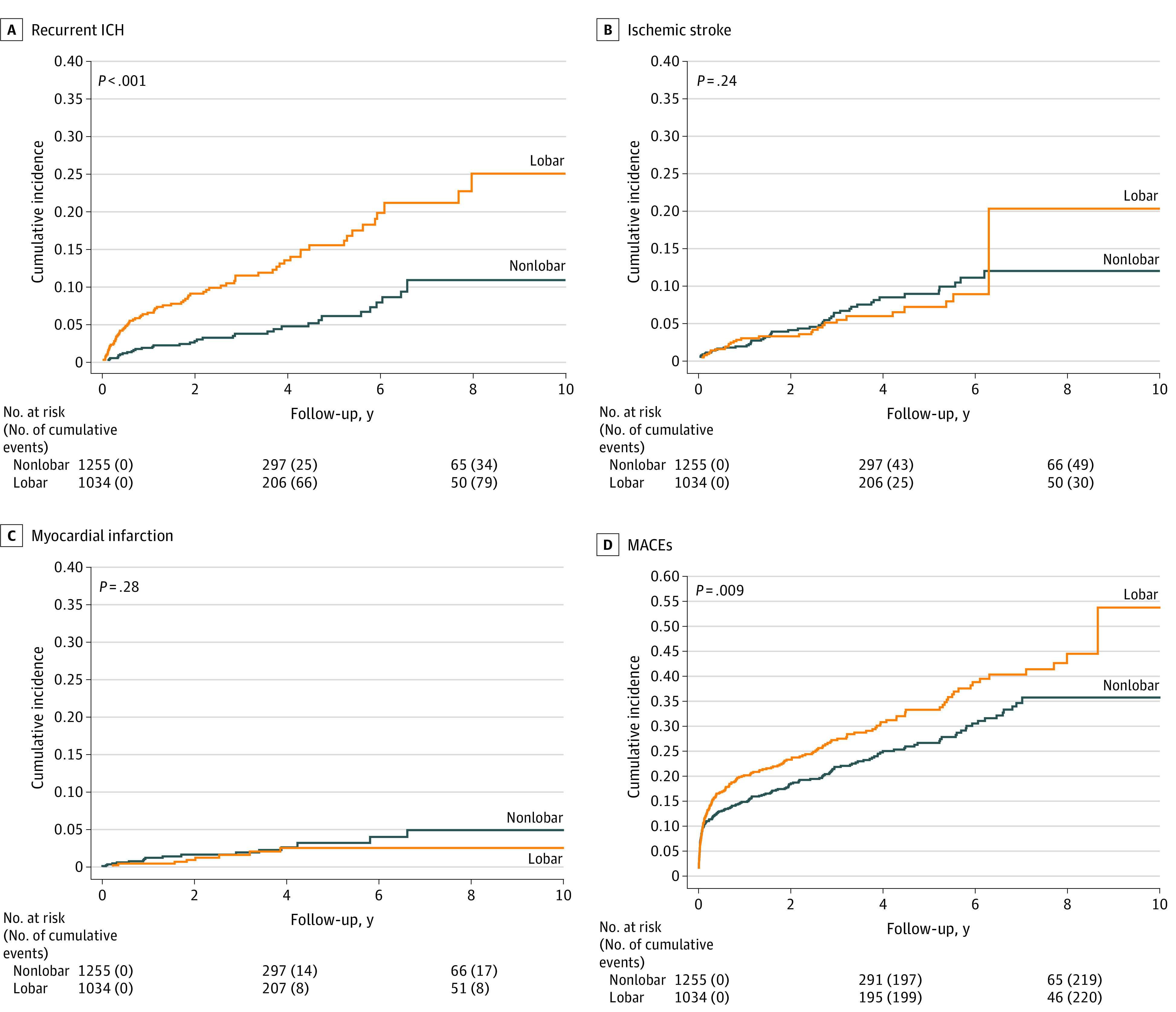
Objective: To examine the risk of MACEs (ie, the composite of ICH, IS, spontaneous intracranial extra-axial hemorrhage, MI, systemic embolism, or vascular death) after ICH based on ICH location (lobar vs nonlobar).
Design, setting, and participants: This cohort study identified 2819 patients in southern Denmark (population of 1.2 million) 50 years or older hospitalized with first-ever spontaneous ICH from January 1, 2009, to December 31, 2018. Intracerebral hemorrhage was categorized as lobar or nonlobar, and the cohorts were linked to registry data until the end of 2018 to identify the occurrence of MACEs and separately recurrent ICH, IS, and MI. Outcome events were validated using medical records. Associations were adjusted for potential confounders using inverse probability weighting.
Exposure: Location of ICH (lobar vs nonlobar).
Main outcomes and measures: The main outcomes were MACEs and separately recurrent ICH, IS, and MI. Crude absolute event rates per 100 person-years and adjusted hazard ratios (aHRs) with 95% CIs were calculated. Data were analyzed from February to September 2022.
Results: Compared with patients with nonlobar ICH (n = 1255; 680 [54.2%] men and 575 [45.8%] women; mean [SD] age, 73.5 [11.4] years), those with lobar ICH (n = 1034; 495 [47.9%] men and 539 [52.1%] women, mean [SD] age, 75.2 [10.7] years) had higher rates of MACEs per 100 person-years (10.84 [95% CI, 9.51-12.37] vs 7.91 [95% CI, 6.93-9.03]; aHR, 1.26; 95% CI, 1.10-1.44) and recurrent ICH (3.74 [95% CI, 3.01-4.66] vs 1.24 [95% CI, 0.89-1.73]; aHR, 2.63; 95% CI, 1.97-3.49) but not IS (1.45 [95% CI, 1.02-2.06] vs 1.77 [95% CI, 1.34-2.34]; aHR, 0.81; 95% CI, 0.60-1.10) or MI (0.42 [95% CI, 0.22-0.81] vs 0.64 [95% CI, 0.40-1.01]; aHR, 0.64; 95% CI, 0.38-1.09).
Conclusions and relevance: In this cohort study, spontaneous lobar ICH was associated with a higher rate of subsequent MACEs than nonlobar ICH, primarily due to a higher rate of recurrent ICH. This study highlights the importance of secondary ICH prevention strategies in patients with lobar ICH.
Conflict of interest statement
Figures
Comment in
-
Major Adverse Cardiovascular Events After Intracerebral Hemorrhage-It's All About Location, Location, Location.JAMA Netw Open. 2023 Apr 3;6(4):e235783. doi: 10.1001/jamanetworkopen.2023.5783. JAMA Netw Open. 2023. PMID: 37017973 No abstract available.
