

Asymmetric Hearing Loss in Adult Cochlear Implant Recipients: Results and Recommendations From a Multisite Prospective Clinical Trial
- PMID: 37018114
- PMCID: PMC10440208
- DOI: 10.1097/AUD.0000000000001354
Asymmetric Hearing Loss in Adult Cochlear Implant Recipients: Results and Recommendations From a Multisite Prospective Clinical Trial
Abstract
Objective: A multisite clinical trial was conducted to obtain cochlear implant (CI) efficacy data in adults with asymmetric hearing loss (AHL) and establish an evidence-based framework for clinical decision-making regarding CI candidacy, counseling, and assessment tools. Study hypotheses were threefold: (1) 6-month postimplant performance in the poor ear (PE) with a CI will be significantly better than preimplant performance with a hearing aid (HA), (2) 6-month postimplant performance with a CI and HA (bimodal) will be significantly better than preimplant performance with bilateral HAs (Bil HAs), and (3) 6-month postimplant bimodal performance will be significantly better than aided, better ear (BE) performance.
Design: Forty adults with AHL from four, metropolitan CI centers participated. Hearing criteria for the ear to be implanted included (1) pure-tone average (PTA, 0.5, 1, 2 kHz) of >70 dB HL, (2) aided, monosyllabic word score of ≤30%, (3) duration of severe-to-profound hearing loss of ≥6 months, and (4) onset of hearing loss ≥6 years of age. Hearing criteria for the BE included (1) PTA (0.5, 1, 2, 4 kHz) of 40 to 70 dB HL, (2) currently using a HA, (3) aided, word score of >40%, and (4) stable hearing for the previous 1-year period. Speech perception and localization measures, in quiet and in noise, were administered preimplant and at 3-, 6-, 9-, and 12-months postimplant. Preimplant testing was performed in three listening conditions, PE HA, BE HA, and Bil HAs. Postimplant testing was performed in three conditions, CI, BE HA, and bimodal. Outcome factors included age at implantation and length of deafness (LOD) in the PE.
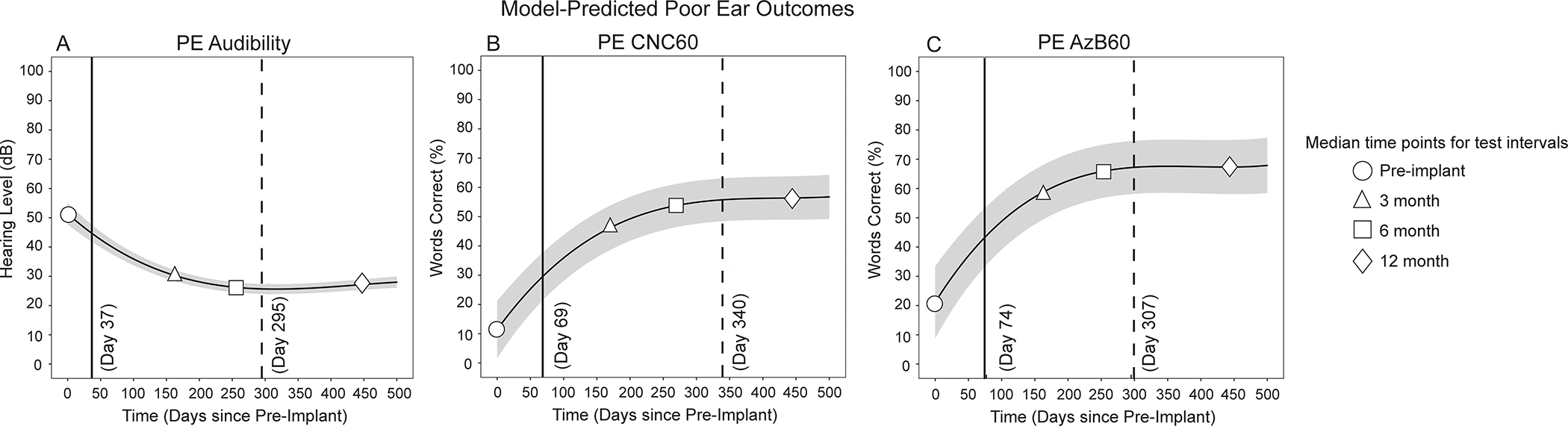
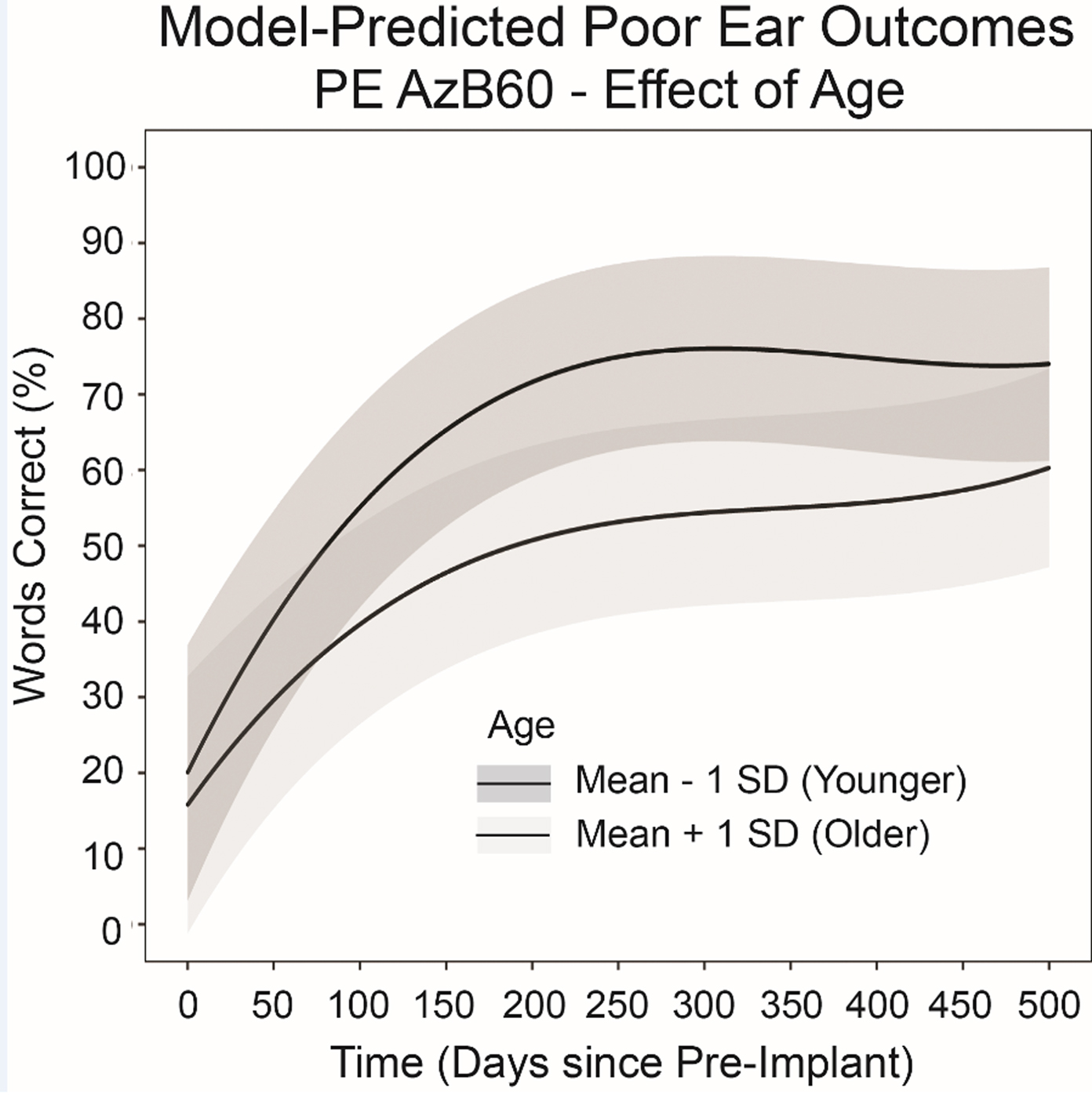
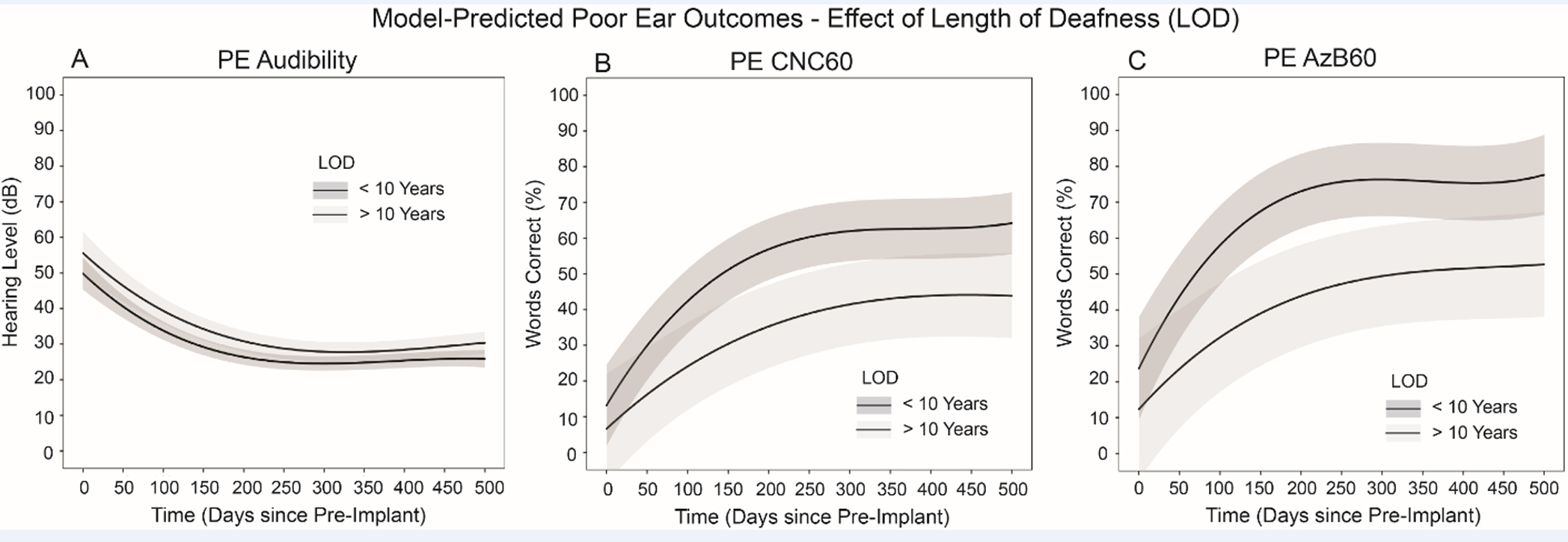
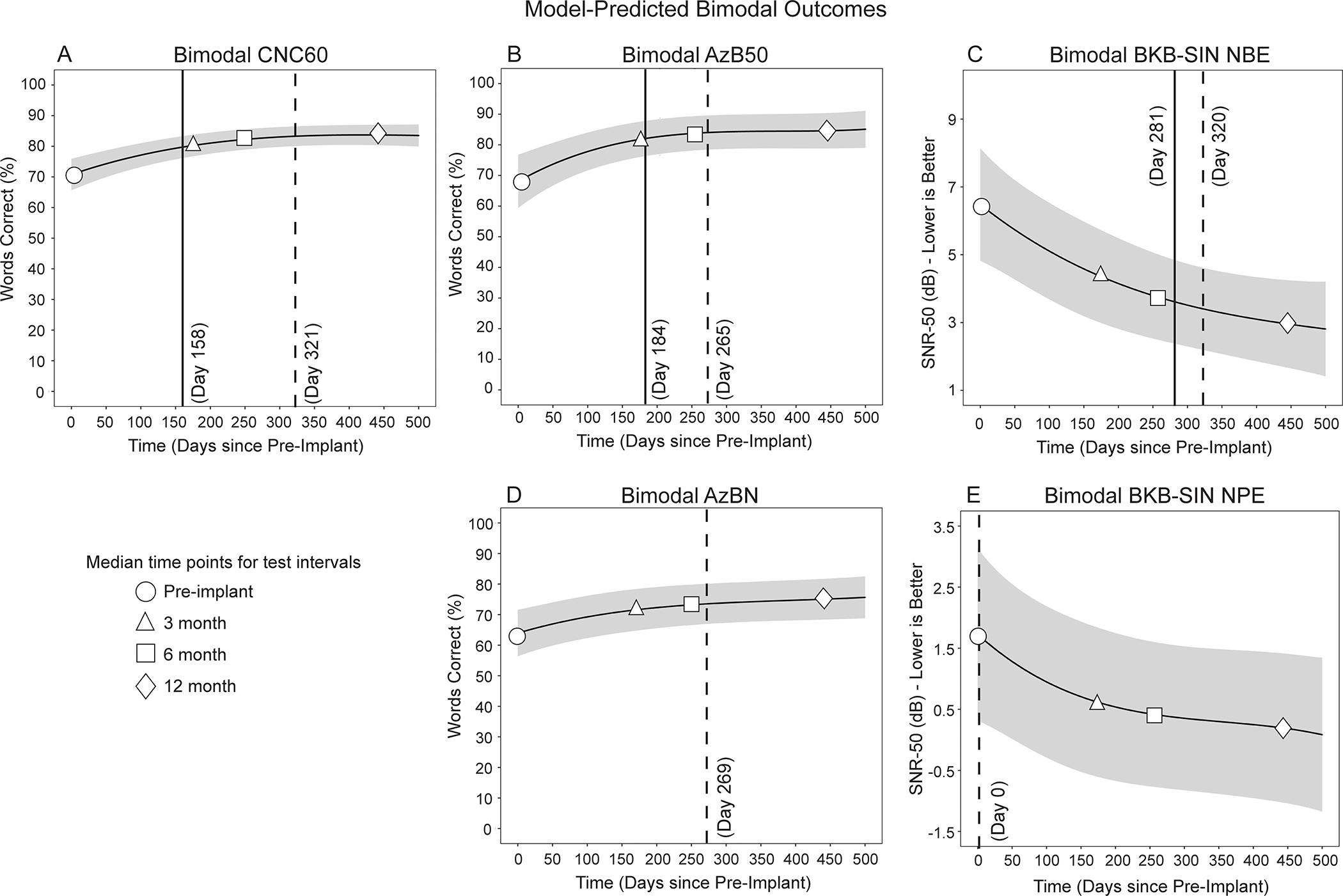
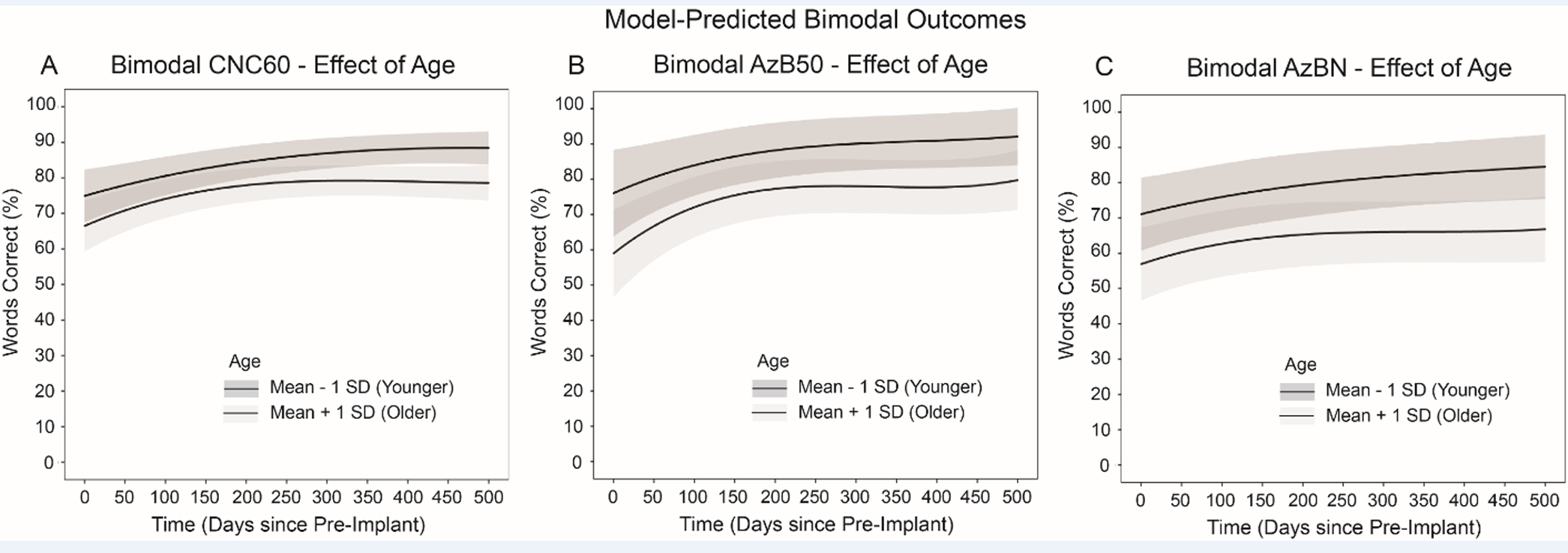
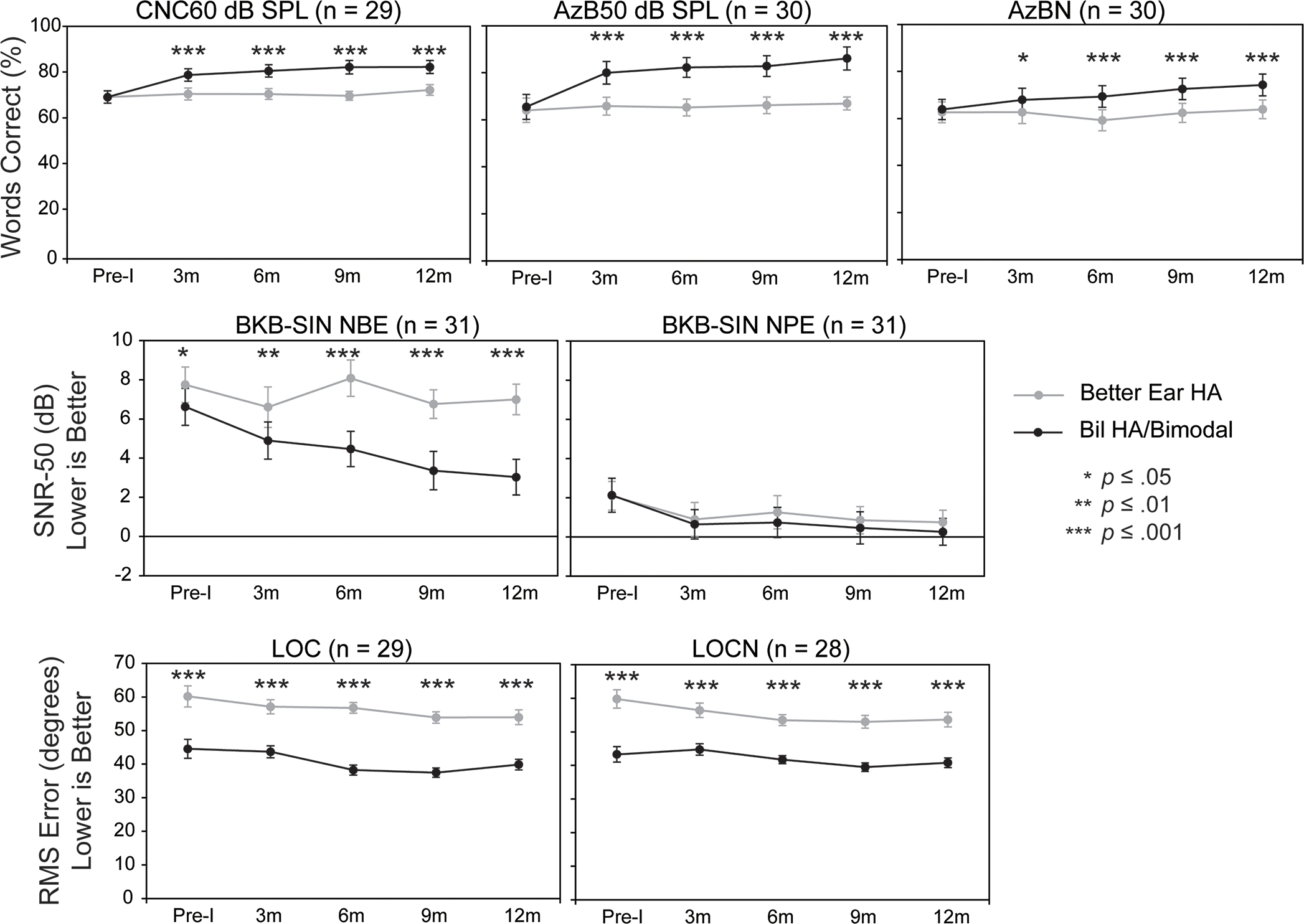
Results: A hierarchical nonlinear analysis predicted significant improvement in the PE by 3 months postimplant versus preimplant for audibility and speech perception with a plateau in performance at approximately 6 months. The model predicted significant improvement in postimplant, bimodal outcomes versus preimplant outcomes (Bil HAs) for all speech perception measures by 3 months. Both age and LOD were predicted to moderate some CI and bimodal outcomes. In contrast with speech perception, localization in quiet and noise was not predicted to improve by 6 months when comparing Bil HAs (preimplant) to bimodal (postimplant) outcomes. However, when participants' preimplant everyday listening condition (BE HA or Bil HAs) was compared with bimodal performance, the model predicted significant improvement by 3 months for localization in quiet and noise. Lastly, BE HA results were stable over time; a generalized linear model analysis revealed bimodal performance was significantly better than performance with a BE HA at all postimplant intervals for most speech perception measures and localization.
Conclusions: Results revealed significant CI and bimodal benefit for AHL participants by 3-months postimplant, with a plateau in CI and bimodal performance at approximately 6-months postimplant. Results can be used to inform AHL CI candidates and to monitor postimplant performance. On the basis of this and other AHL research, clinicians should consider a CI for individuals with AHL if the PE has a PTA (0.5, 1, 2 kHz) >70 dB HL and a Consonant-Vowel Nucleus-Consonant word score ≤40%. LOD >10 years should not be a contraindication.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Results in Adult Cochlear Implant Recipients With Varied Asymmetric Hearing: A Prospective Longitudinal Study of Speech Recognition, Localization, and Participant Report.Ear Hear. 2018 Sep/Oct;39(5):845-862. doi: 10.1097/AUD.0000000000000548. Ear Hear. 2018. PMID: 29373326 Free PMC article.
-
Longitudinal outcomes of cochlear implantation and bimodal hearing in a large group of adults: A multicenter clinical study.Am J Otolaryngol. 2021 Jan-Feb;42(1):102773. doi: 10.1016/j.amjoto.2020.102773. Epub 2020 Oct 22. Am J Otolaryngol. 2021. PMID: 33161258
-
Cochlear implantation in adults with asymmetric hearing loss.Ear Hear. 2012 Jul-Aug;33(4):521-33. doi: 10.1097/AUD.0b013e31824b9dfc. Ear Hear. 2012. PMID: 22441359 Free PMC article.
-
Implantable Devices for Single-Sided Deafness and Conductive or Mixed Hearing Loss: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Mar 6;20(1):1-165. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 32194878 Free PMC article.
-
Identification of Pure-Tone Audiologic Thresholds for Pediatric Cochlear Implant Candidacy: A Systematic Review.JAMA Otolaryngol Head Neck Surg. 2018 Jul 1;144(7):630-638. doi: 10.1001/jamaoto.2018.0652. JAMA Otolaryngol Head Neck Surg. 2018. PMID: 29800000
Cited by
-
State-of-the-Art on the Impact of Bimodal Acoustic Stimulation on Speech Perception in Noise in Adults: A Systematic Review.Audiol Res. 2024 Oct 16;14(5):914-927. doi: 10.3390/audiolres14050077. Audiol Res. 2024. PMID: 39452469 Free PMC article. Review.
-
Evaluation of medium-term cochlear implant use in patients with asymmetric hearing loss.Eur Arch Otorhinolaryngol. 2025 Apr 16. doi: 10.1007/s00405-025-09366-0. Online ahead of print. Eur Arch Otorhinolaryngol. 2025. PMID: 40240700
References
-
- Arndt S, Aschendorff A, Laszig R, Beck R, Schild C, Kroeger S, … Wesarg T (2011). Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol Neurotol, 32(1), 39–47. 10.1097/MAO.0b013e3181fcf271 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
