

Noninvasive respiratory support after extubation: a systematic review and network meta-analysis
- PMID: 37019458
- PMCID: PMC10074166
- DOI: 10.1183/16000617.0196-2022
Noninvasive respiratory support after extubation: a systematic review and network meta-analysis
Erratum in
-
"Noninvasive respiratory support after extubation: a systematic review and network meta-analysis". A. Boscolo, T. Pettenuzzo, N. Sella, M. Zatta, M. Salvagno, M. Tassone, C. Pretto, A. Peralta, L. Muraro, F. Zarantonello, A. Bruni, F. Geraldini, A. De Cassai and P. Navalesi. Eur Respir Rev 2023; 32: 220196.Eur Respir Rev. 2023 Jun 21;32(168):225196. doi: 10.1183/16000617.5196-2022. Print 2023 Jun 30. Eur Respir Rev. 2023. PMID: 37343963 Free PMC article. No abstract available.
Abstract
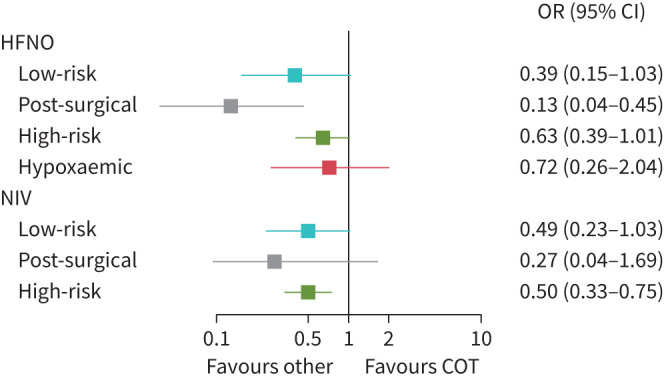
Background: The effect of noninvasive respiratory support (NRS), including high-flow nasal oxygen, bi-level positive airway pressure and continuous positive airway pressure (noninvasive ventilation (NIV)), for preventing and treating post-extubation respiratory failure is still unclear. Our objective was to assess the effects of NRS on post-extubation respiratory failure, defined as re-intubation secondary to post-extubation respiratory failure (primary outcome). Secondary outcomes included the incidence of ventilator-associated pneumonia (VAP), discomfort, intensive care unit (ICU) and hospital mortality, ICU and hospital length of stay (LOS), and time to re-intubation. Subgroup analyses considered "prophylactic" versus "therapeutic" NRS application and subpopulations (high-risk, low-risk, post-surgical and hypoxaemic patients).
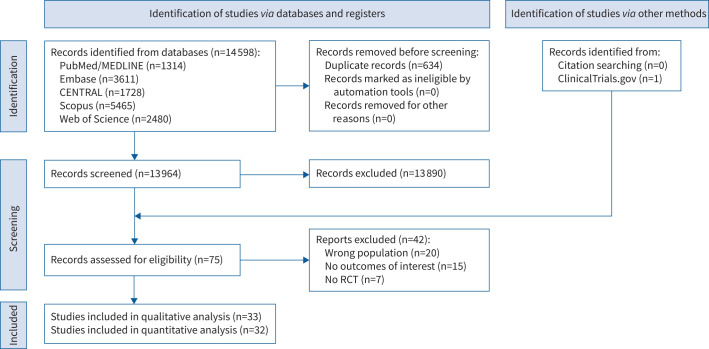
Methods: We undertook a systematic review and network meta-analysis (Research Registry: reviewregistry1435). PubMed, Embase, CENTRAL, Scopus and Web of Science were searched (from inception until 22 June 2022). Randomised controlled trials (RCTs) investigating the use of NRS after extubation in ICU adult patients were included.
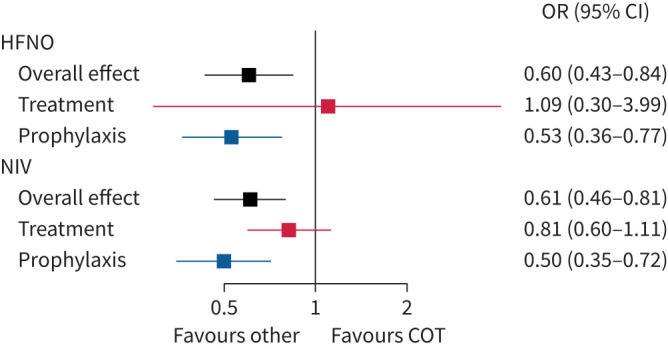
Results: 32 RCTs entered the quantitative analysis (5063 patients). Compared with conventional oxygen therapy, NRS overall reduced re-intubations and VAP (moderate certainty). NIV decreased hospital mortality (moderate certainty), and hospital and ICU LOS (low and very low certainty, respectively), and increased discomfort (moderate certainty). Prophylactic NRS did not prevent extubation failure in low-risk or hypoxaemic patients.
Conclusion: Prophylactic NRS may reduce the rate of post-extubation respiratory failure in ICU patients.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: None related to the present work. P. Navalesi's research lab has received grants/research equipment from Draeger, Intersurgical SPA and Gilead. P. Navalesi receives royalties from Intersurgical SPA for the Helmet Next invention. He has also received speaking fees from Getinge, Intersurgical SPA, Mindray, Gilead, MSD, Draeger and Medicair. The other authors have no other competing interests to declare.
Figures
Comment in
-
New insights into acute and chronic respiratory failure: highlights from the Respiratory Failure and Mechanical Ventilation Conference 2022.Eur Respir Rev. 2023 Apr 5;32(168):230027. doi: 10.1183/16000617.0027-2023. Print 2023 Jun 30. Eur Respir Rev. 2023. PMID: 37019460 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical