

Sleep Patterns and the Risk of Acute Stroke: Results From the INTERSTROKE International Case-Control Study
- PMID: 37019662
- PMCID: PMC10238154
- DOI: 10.1212/WNL.0000000000207249
Sleep Patterns and the Risk of Acute Stroke: Results From the INTERSTROKE International Case-Control Study
Abstract
Background and objectives: Symptoms of sleep disturbance are common and may represent important modifiable risk factors of stroke. We evaluated the association between a spectrum of sleep disturbance symptoms and the risk of acute stroke in an international setting.
Methods: The INTERSTROKE study is an international case-control study of patients presenting with first acute stroke and controls matched by age (±5 years) and sex. Sleep symptoms in the previous month were assessed through a questionnaire. Conditional logistic regression estimated the association between sleep disturbance symptoms and acute stroke, expressed as odds ratios (ORs) and 95% CIs. The primary model adjusted for age, occupation, marital status, and modified Rankin scale at baseline, with subsequent models adjusting for potential mediators (behavioral/disease risk factors).
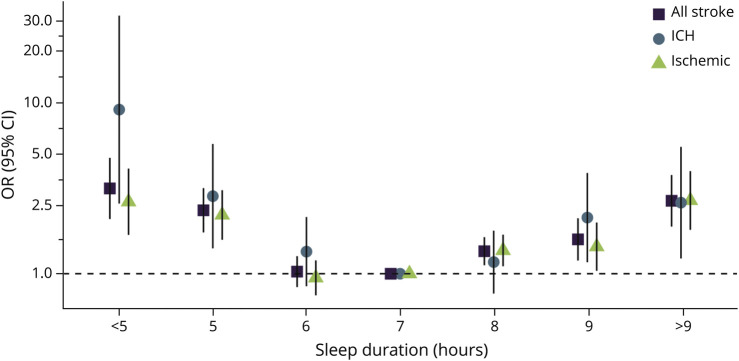
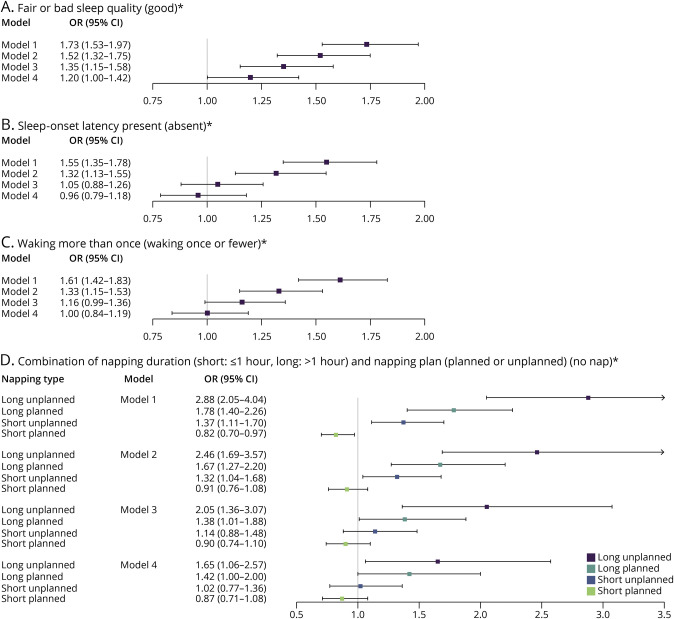
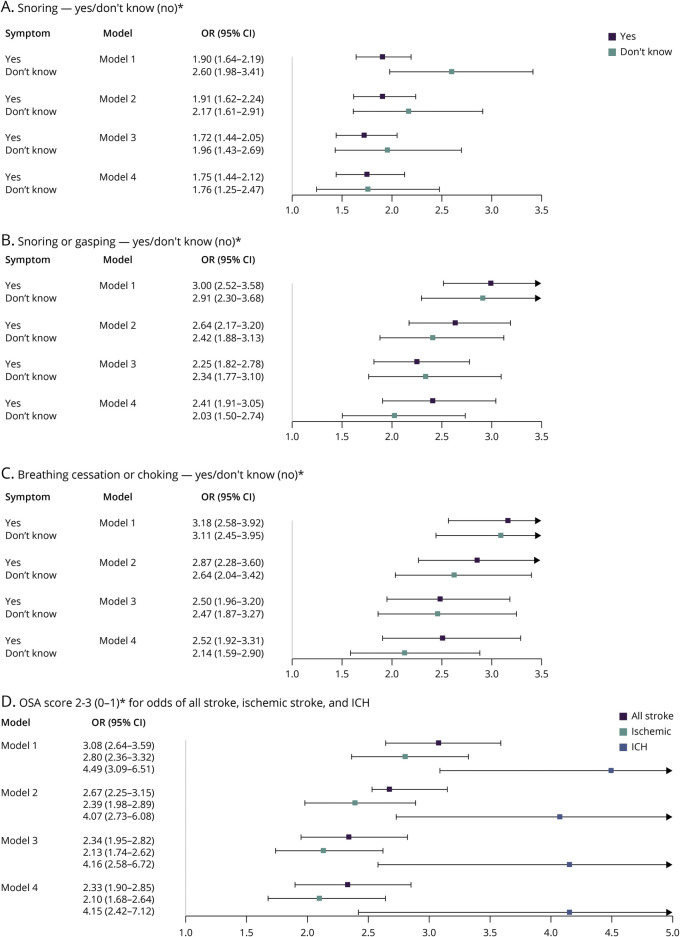
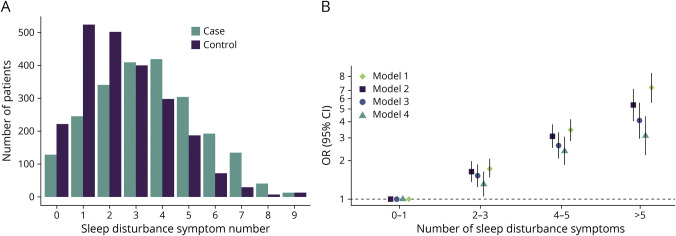
Results: Overall, 4,496 matched participants were included, with 1,799 of them having experienced an ischemic stroke and 439 an intracerebral hemorrhage. Short sleep (<5 hours: OR 3.15, 95% CI 2.09-4.76), long sleep (>9 hours: OR 2.67, 95% CI 1.89-3.78), impaired quality (OR 1.52, 95% CI 1.32-1.75), difficulty getting to sleep (OR 1.32, 95% CI 1.13-1.55) or maintaining sleep (OR 1.33, 95% CI 1.15-1.53), unplanned napping (OR 1.48, 95% CI 1.20-1.84), prolonged napping (>1 hour: OR 1.88, 95% CI 1.49-2.38), snoring (OR 1.91, 95% CI 1.62-2.24), snorting (OR 2.64, 95% CI 2.17-3.20), and breathing cessation (OR 2.87, 95% CI 2.28-3.60) were all significantly associated with an increased odds of acute stroke in the primary model. A derived obstructive sleep apnea score of 2-3 (2.67, 2.25-3.15) and cumulative sleep symptoms (>5: 5.38, 4.03-7.18) were also associated with a significantly increased odds of acute stroke, with the latter showing a graded association. After an extensive adjustment, significance was maintained for most of the symptoms (not difficulty getting to/maintaining sleep and unplanned napping), with similar findings for stroke subtypes.
Discussion: We found that sleep disturbance symptoms were common and associated with a graded increased risk of stroke. These symptoms may be a marker of increased individual risk or represent independent risk factors. Future clinical trials are warranted to determine the efficacy of sleep interventions in stroke prevention.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no disclosures relevant to the manuscript. Go to
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical