

Post-reperfusion acute MR diffusion in stroke is a potential predictor for clinical outcome in rats
- PMID: 37019923
- PMCID: PMC10076321
- DOI: 10.1038/s41598-023-32679-1
Post-reperfusion acute MR diffusion in stroke is a potential predictor for clinical outcome in rats
Abstract
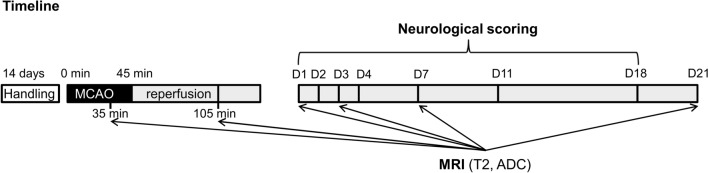
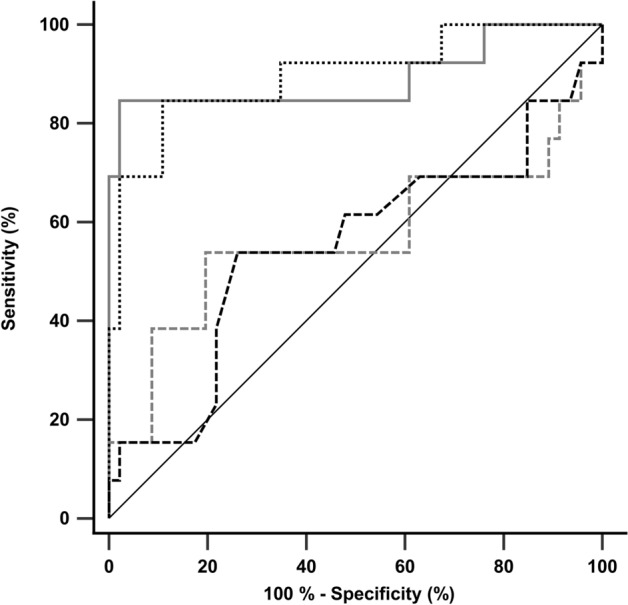
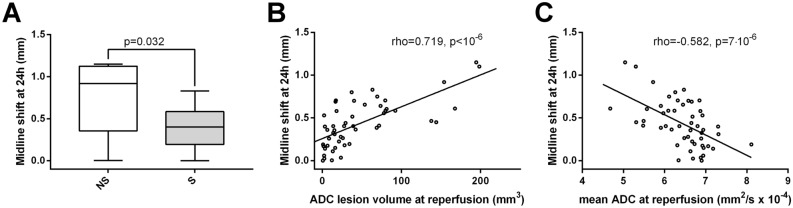
Middle cerebral artery occlusion (MCAO) models show substantial variability in outcome, introducing uncertainties in the evaluation of treatment effects. Early outcome predictors would be essential for prognostic purposes and variability control. We aimed to compare apparent diffusion coefficient (ADC) MRI data obtained during MCAO and shortly after reperfusion for their potentials in acute-phase outcome prediction. Fifty-nine male rats underwent a 45-min MCAO. Outcome was defined in three ways: 21-day survival; 24 h midline-shift and neurological scores. Animals were divided into two groups: rats surviving 21 days after MCAO (survival group, n = 46) and rats dying prematurely (non-survival/NS group, n = 13). At reperfusion, NS group showed considerably larger lesion volume and lower mean ADC of the initial lesion site (p < 0.0001), while during occlusion there were no significant group differences. At reperfusion, each survival animal showed decreased lesion volume and increased mean ADC of the initial lesion site compared to those during occlusion (p < 10-6), while NS group showed a mixed pattern. At reperfusion, lesion volume and mean ADC of the initial lesion site were significantly associated with 24 h midline-shift and neurological scores. Diffusion MRI performed soon after reperfusion has a great impact in early-phase outcome prediction, and it works better than the measurement during occlusion.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
