

Clinical applications of photon counting detector CT
- PMID: 37020069
- PMCID: PMC10330165
- DOI: 10.1007/s00330-023-09596-y
Clinical applications of photon counting detector CT
Abstract
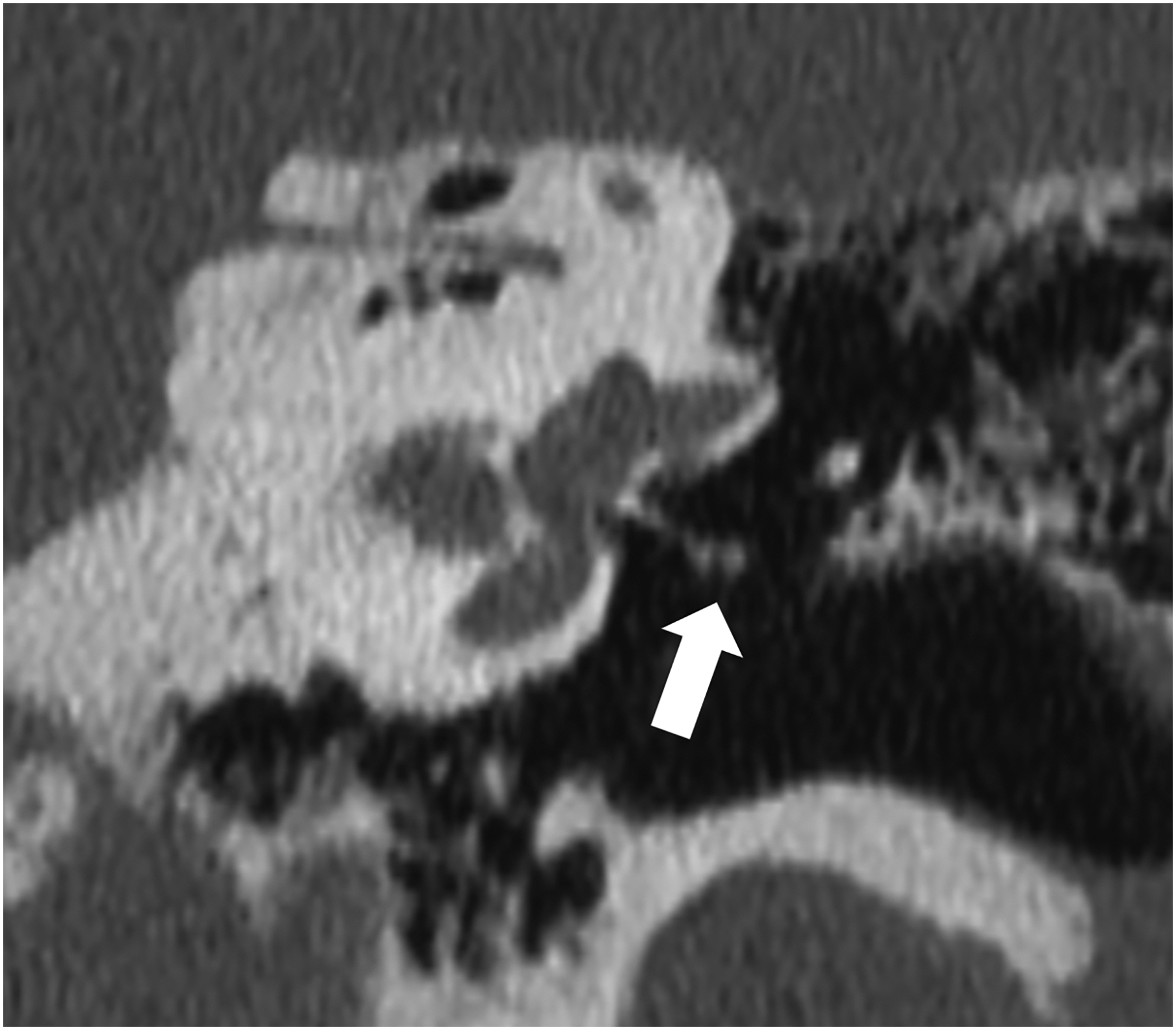
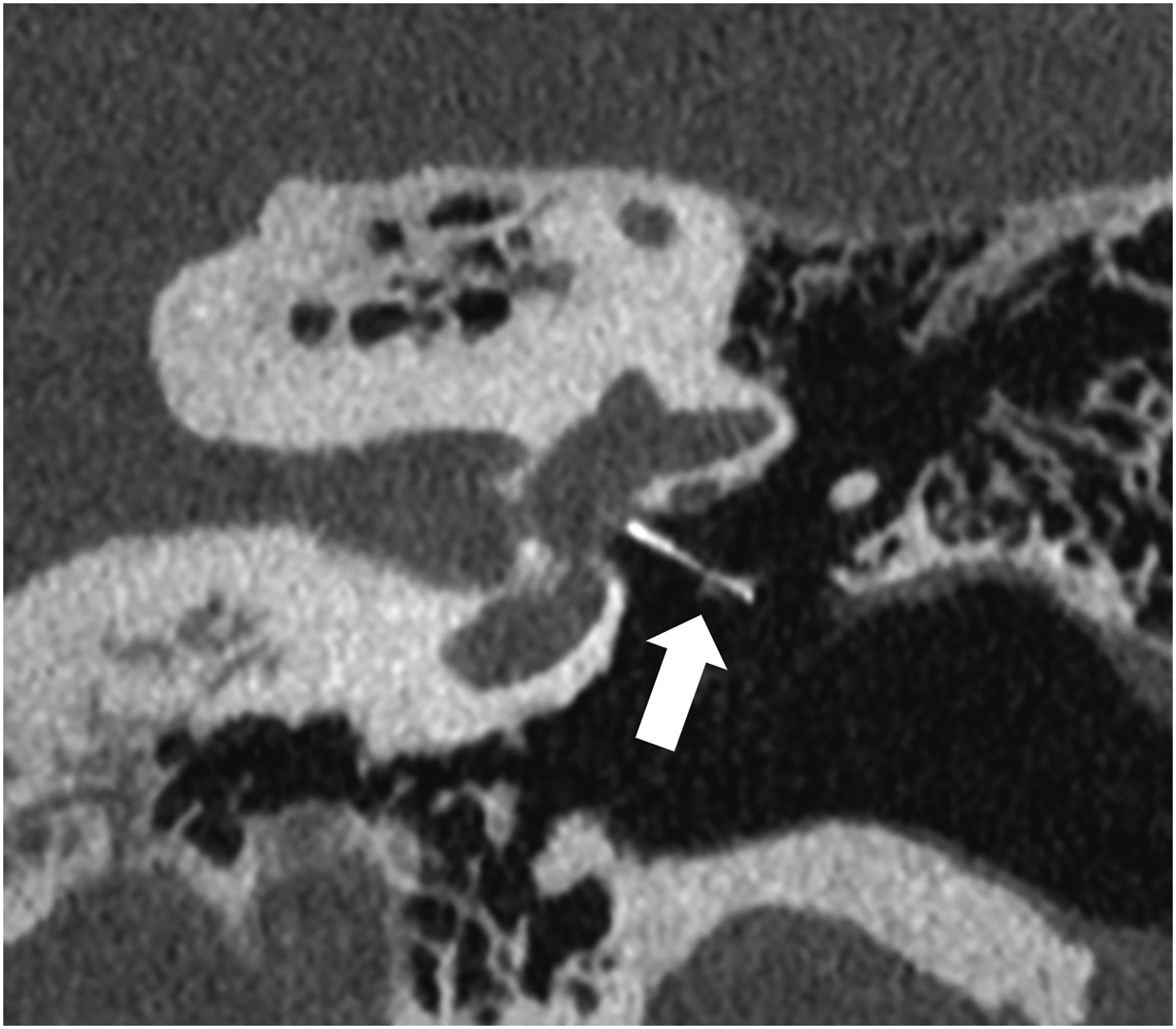
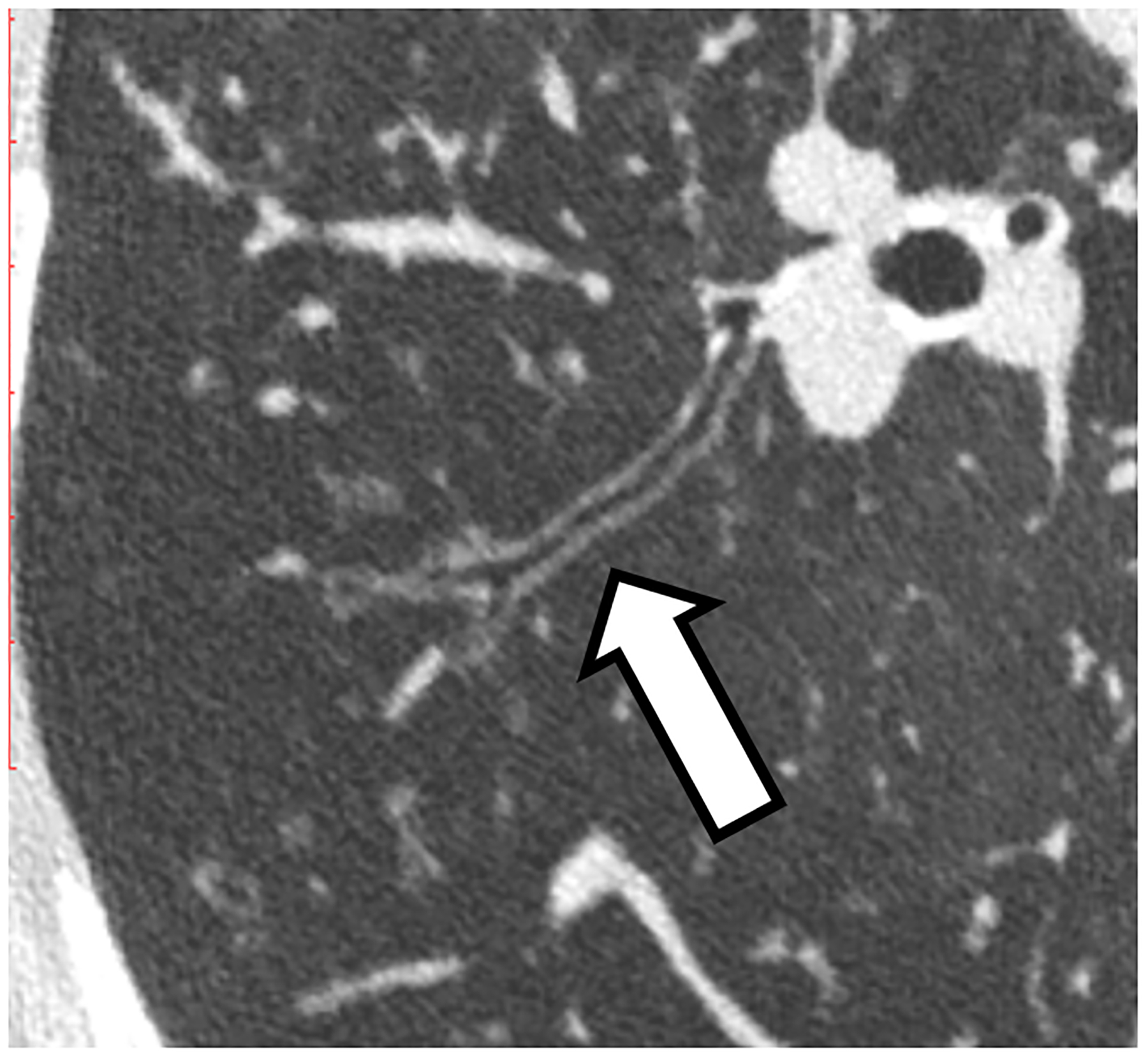
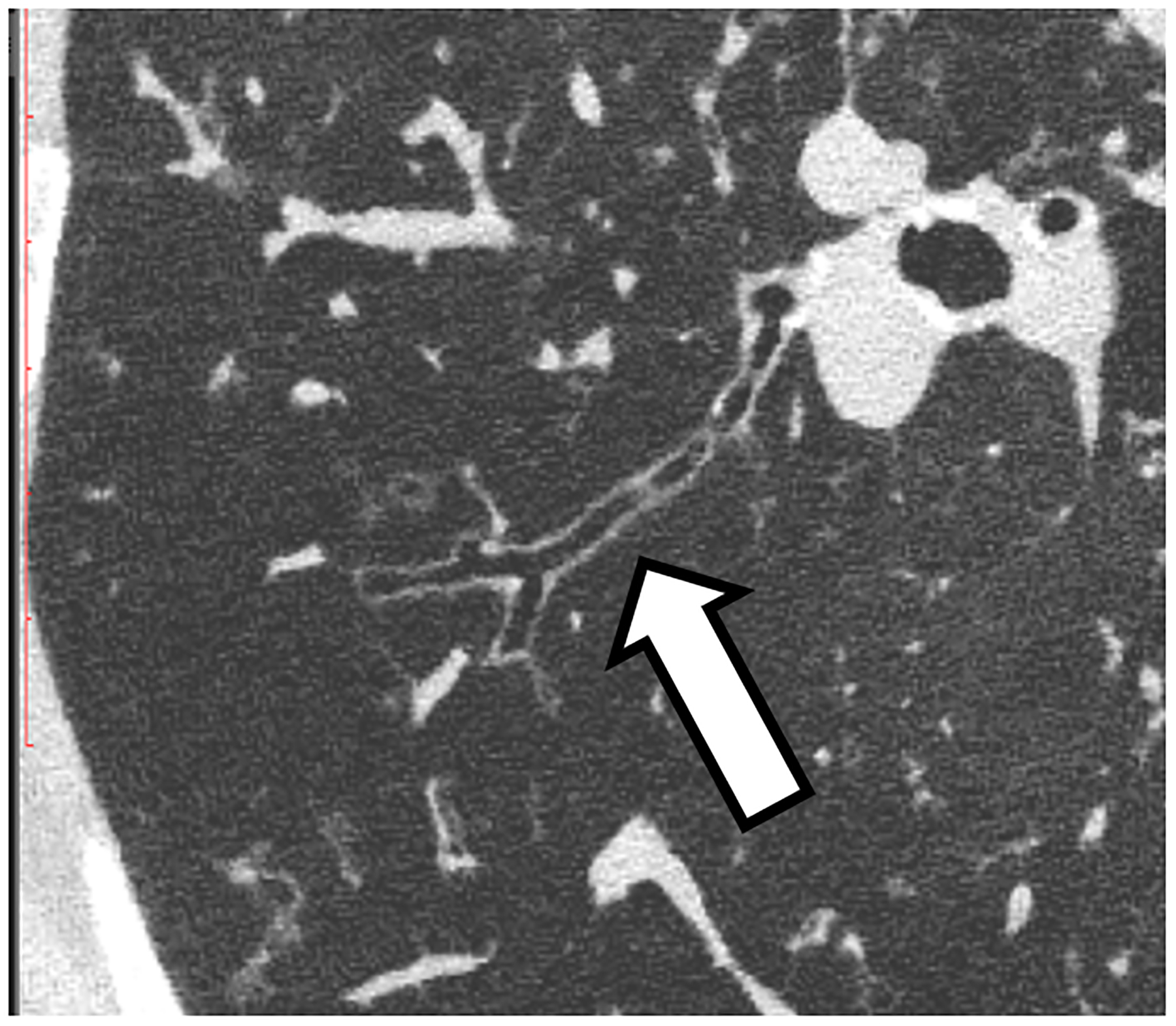
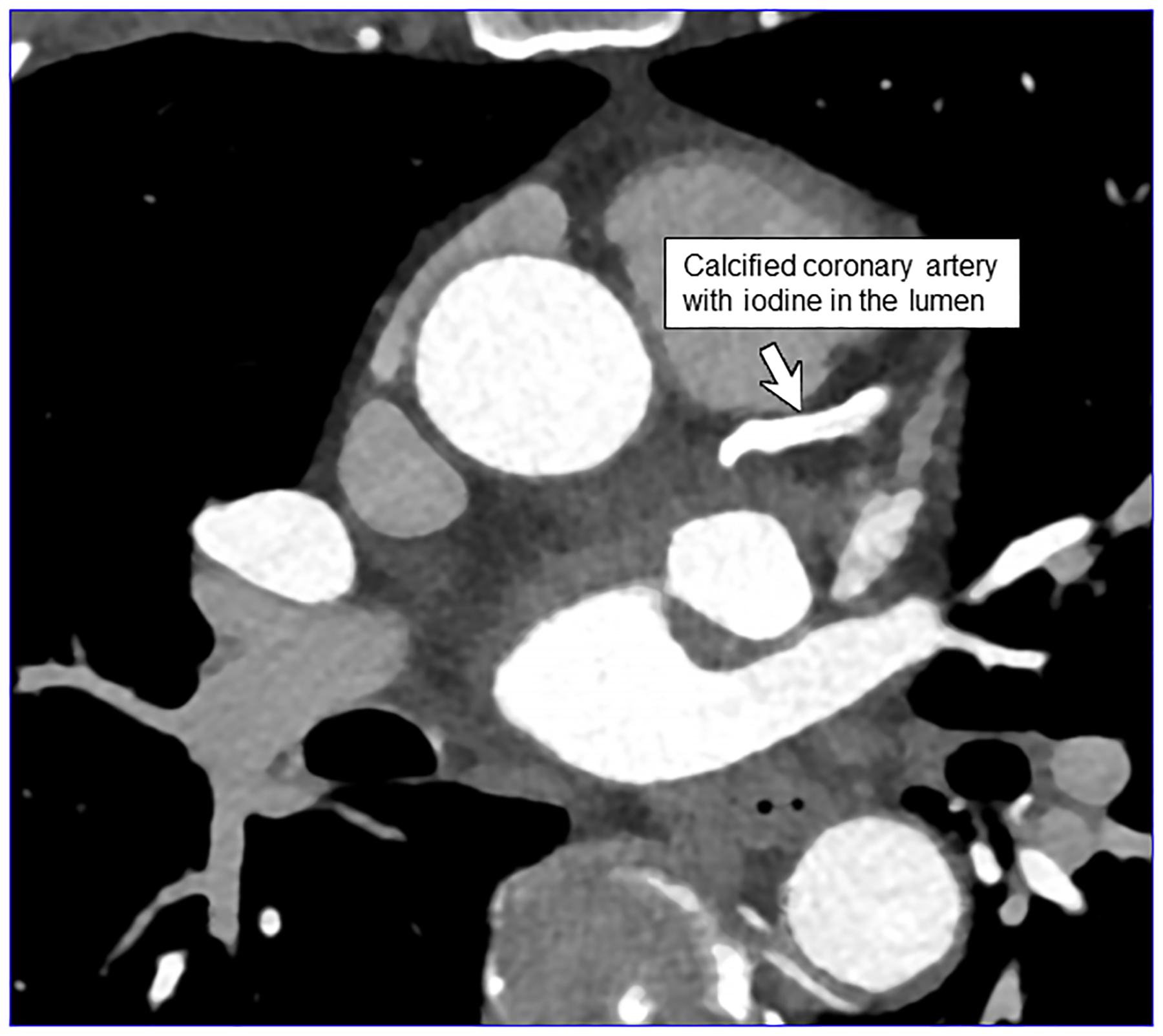
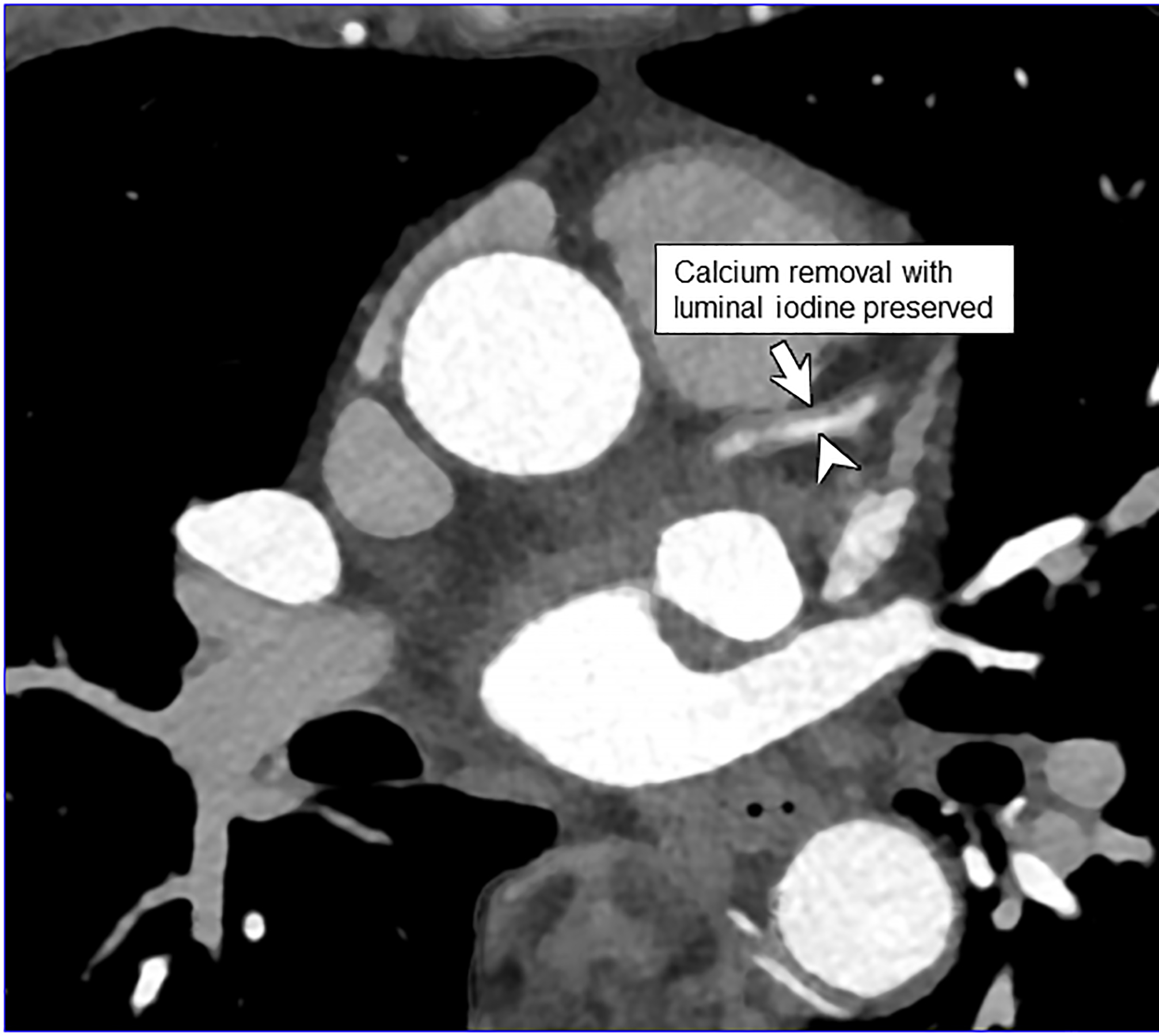
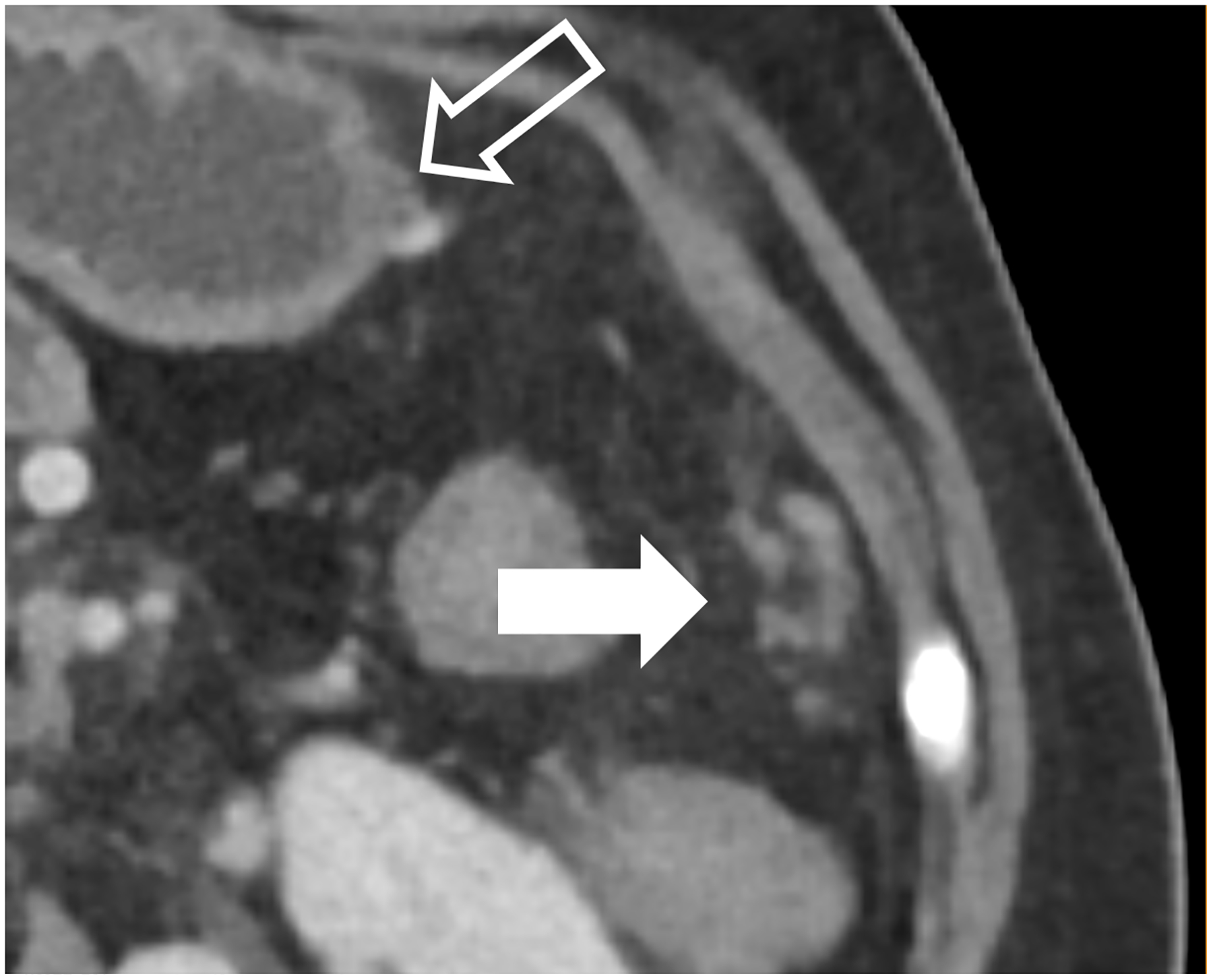
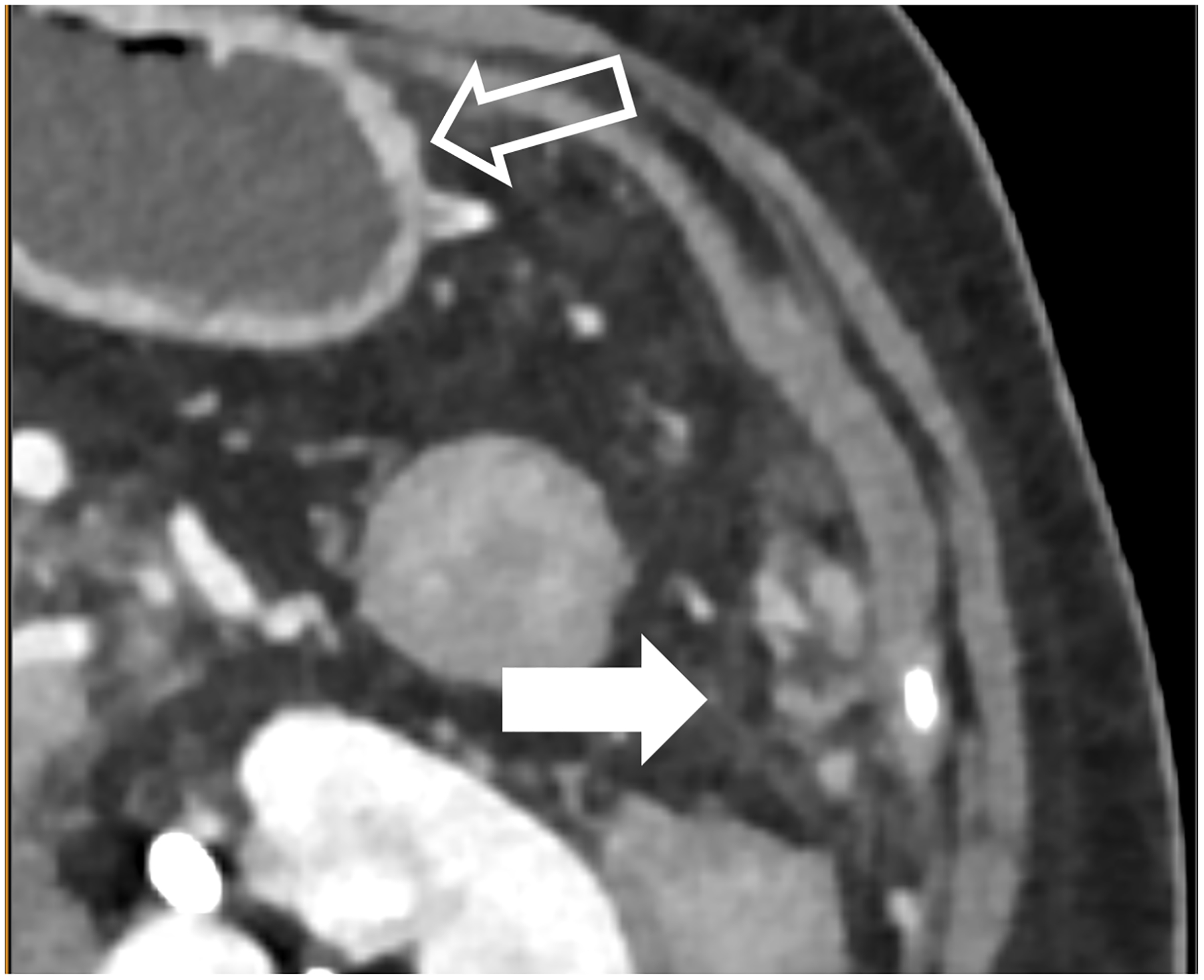
The X-ray detector is a fundamental component of a CT system that determines the image quality and dose efficiency. Until the approval of the first clinical photon-counting-detector (PCD) system in 2021, all clinical CT scanners used scintillating detectors, which do not capture information about individual photons in the two-step detection process. In contrast, PCDs use a one-step process whereby X-ray energy is converted directly into an electrical signal. This preserves information about individual photons such that the numbers of X-ray in different energy ranges can be counted. Primary advantages of PCDs include the absence of electronic noise, improved radiation dose efficiency, increased iodine signal and the ability to use lower doses of iodinated contrast material, and better spatial resolution. PCDs with more than one energy threshold can sort the detected photons into two or more energy bins, making energy-resolved information available for all acquisitions. This allows for material classification or quantitation tasks to be performed in conjunction with high spatial resolution, and in the case of dual-source CT, high pitch, or high temporal resolution acquisitions. Some of the most promising applications of PCD-CT involve imaging of anatomy where exquisite spatial resolution adds clinical value. These include imaging of the inner ear, bones, small blood vessels, heart, and lung. This review describes the clinical benefits observed to date and future directions for this technical advance in CT imaging. KEY POINTS: • Beneficial characteristics of photon-counting detectors include the absence of electronic noise, increased iodine signal-to-noise ratio, improved spatial resolution, and full-time multi-energy imaging. • Promising applications of PCD-CT involve imaging of anatomy where exquisite spatial resolution adds clinical value and applications requiring multi-energy data simultaneous with high spatial and/or temporal resolution. • Future applications of PCD-CT technology may include extremely high spatial resolution tasks, such as the detection of breast micro-calcifications, and quantitative imaging of native tissue types and novel contrast agents.
Keywords: Humans; Iodine; Photons; Radiation dosage; Tomography, X-ray computed.
© 2023. The Author(s), under exclusive licence to European Society of Radiology.
Figures

References
-
- Benjaminov O, Perlow E, Romman Z et al. (2008) Novel, Energy-Discriminating Photon Counting CT System (EDCT): First Clinical Evaluation—CT Angiography: Carotid Artery StenosisRadiological Society of North America 2008 Scientific Assembly and Annual Meeting, Chicago, Il.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
