

FOLFIRINOX or Gemcitabine-based Chemotherapy for Borderline Resectable and Locally Advanced Pancreatic Cancer: A Multi-institutional, Patient-Level, Meta-analysis and Systematic Review
- PMID: 37020094
- PMCID: PMC10250524
- DOI: 10.1245/s10434-023-13353-2
FOLFIRINOX or Gemcitabine-based Chemotherapy for Borderline Resectable and Locally Advanced Pancreatic Cancer: A Multi-institutional, Patient-Level, Meta-analysis and Systematic Review
Abstract
Background: Pancreatic cancer often presents as locally advanced (LAPC) or borderline resectable (BRPC). Neoadjuvant systemic therapy is recommended as initial treatment. It is currently unclear what chemotherapy should be preferred for patients with BRPC or LAPC.
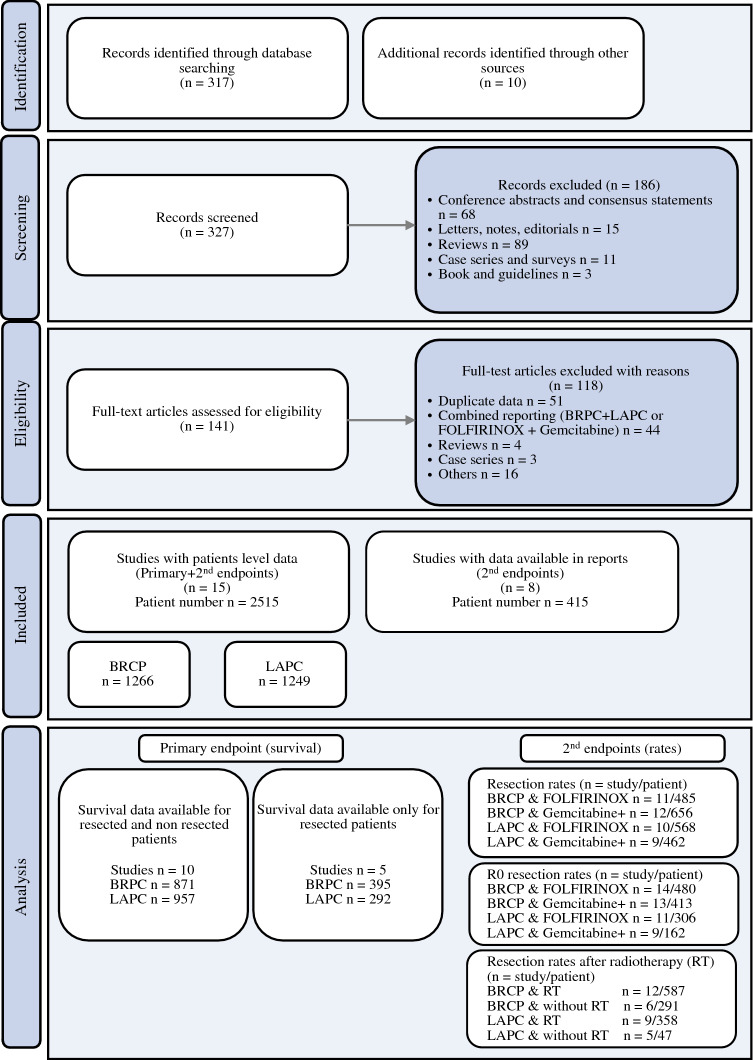
Methods: We performed a systematic review and multi-institutional meta-analysis of patient-level data regarding the use of initial systemic therapy for BRPC and LAPC. Outcomes were reported separately for tumor entity and by chemotherapy regimen including FOLFIRINOX (FIO) or gemcitabine-based.
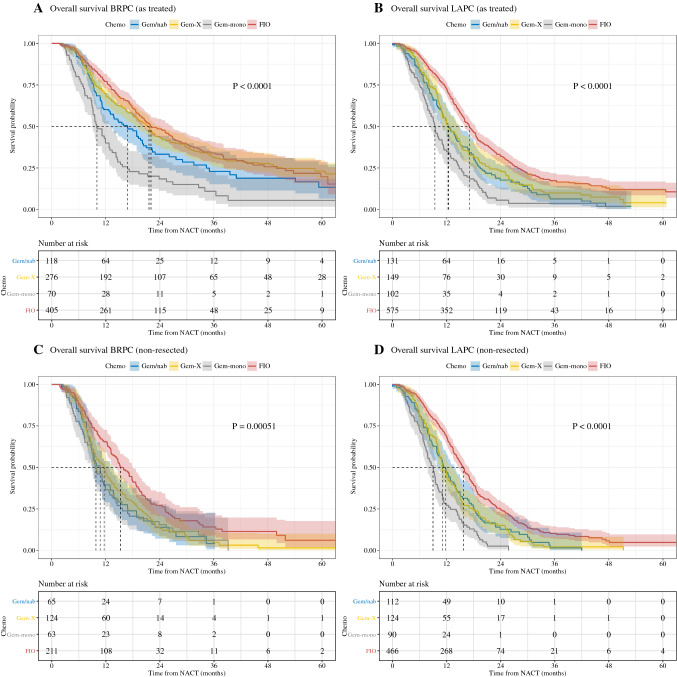
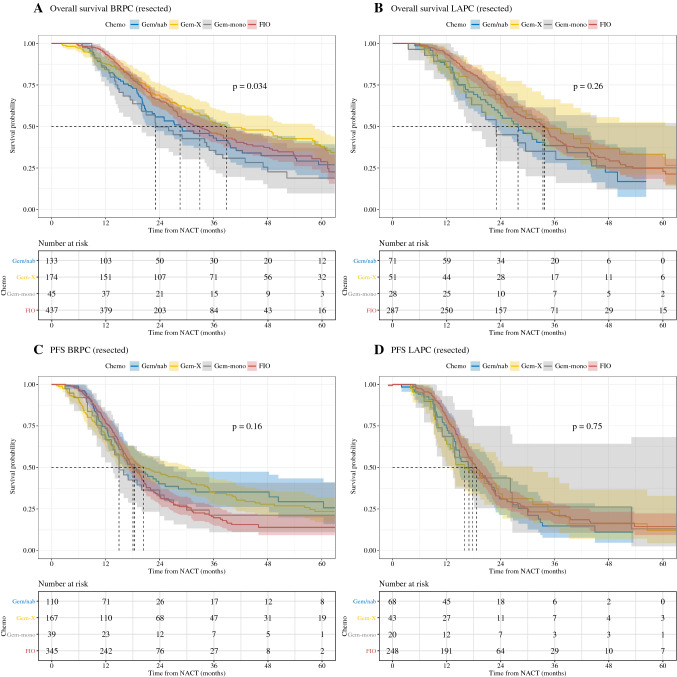
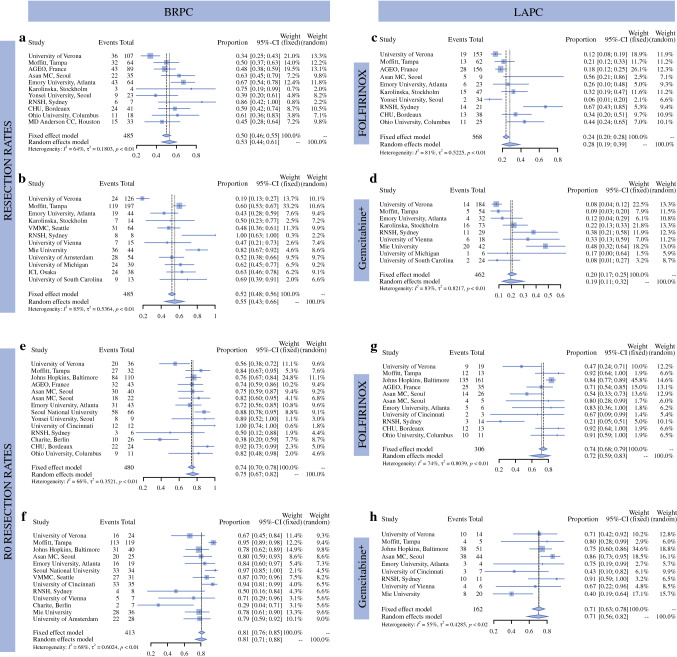
Results: A total of 23 studies comprising 2930 patients were analyzed for overall survival (OS) calculated from the beginning of systemic treatment. OS for patients with BRPC was 22.0 months with FIO, 16.9 months with gemcitabine/nab-paclitaxel (Gem/nab), 21.6 months with gemcitabine/cisplatin or oxaliplatin or docetaxel or capecitabine (GemX), and 10 months with gemcitabine monotherapy (Gem-mono) (p < 0.0001). In patients with LAPC, OS also was higher with FIO (17.1 months) compared with Gem/nab (12.5 months), GemX (12.3 months), and Gem-mono (9.4 months; p < 0.0001). This difference was driven by the patients who did not undergo surgery, where FIO was superior to other regimens. The resection rates for patients with BRPC were 0.55 for gemcitabine-based chemotherapy and 0.53 with FIO. In patients with LAPC, resection rates were 0.19 with Gemcitabine and 0.28 with FIO. In resected patients, OS for patients with BRPC was 32.9 months with FIO and not different compared to Gem/nab, (28.6 months, p = 0.285), GemX (38.8 months, p = 0.1), or Gem-mono (23.1 months, p = 0.083). A similar trend was observed in resected patients converted from LAPC.
Conclusions: In patients with BRPC or LAPC, primary treatment with FOLFIRINOX compared with Gemcitabine-based chemotherapy appears to provide a survival benefit for patients that are ultimately unresectable. For patients that undergo surgical resection, outcomes are similar between GEM+ and FOLFIRINOX when delivered in the neoadjuvant setting.
© 2023. The Author(s).
Figures
Comment in
-
ASO Author Reflections: Chemotherapy Regimen in Borderline Resectable and Locally Advanced Pancreatic Cancer-Resection Cuts the Deal.Ann Surg Oncol. 2023 Jul;30(7):4429-4430. doi: 10.1245/s10434-023-13484-6. Epub 2023 Apr 19. Ann Surg Oncol. 2023. PMID: 37074518 Free PMC article. No abstract available.
References
-
- Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev Clin Oncol. 2010;7(3):163–172. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. - PubMed
-
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goere D, et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v56–68. - PubMed
-
- Tempero MA, Malafa MP, Al-Hawary M, Asbun H, Bain A, Behrman SW, et al. Pancreatic adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(8):1028-61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
