

Application of computed tomography-guided hook-wire localization technique in thoracoscopic surgery for small pulmonary nodules (≤ 10 mm)
- PMID: 37020219
- PMCID: PMC10074372
- DOI: 10.1186/s13019-023-02188-3
Application of computed tomography-guided hook-wire localization technique in thoracoscopic surgery for small pulmonary nodules (≤ 10 mm)
Abstract
Objective: This study aimed to investigate the safety and efficacy of the computed tomography (CT)-guided hook-wire localization technique in thoracoscopic surgery for small pulmonary nodules (≤ 10 mm) and to identify the risk factors for localization-related complications.
Methods: The medical records of 150 patients with small pulmonary nodules treated from January 2018 to June 2021 were retrospectively analyzed. According to preoperative hook-wire positioning status, they were divided into the localization group (50 cases) or the control group (100 cases). The operation time, intraoperative blood loss, hospital stay, and conversion rate to thoracotomy were recorded and compared between groups. Uni- and multivariate binary logistic regression analysis was used to identify the risk factors for localization-related complications.
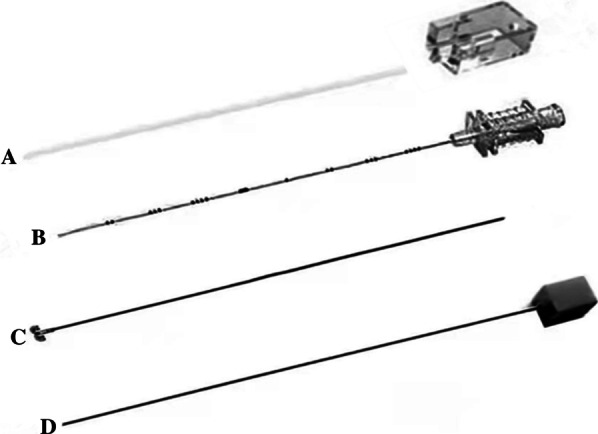
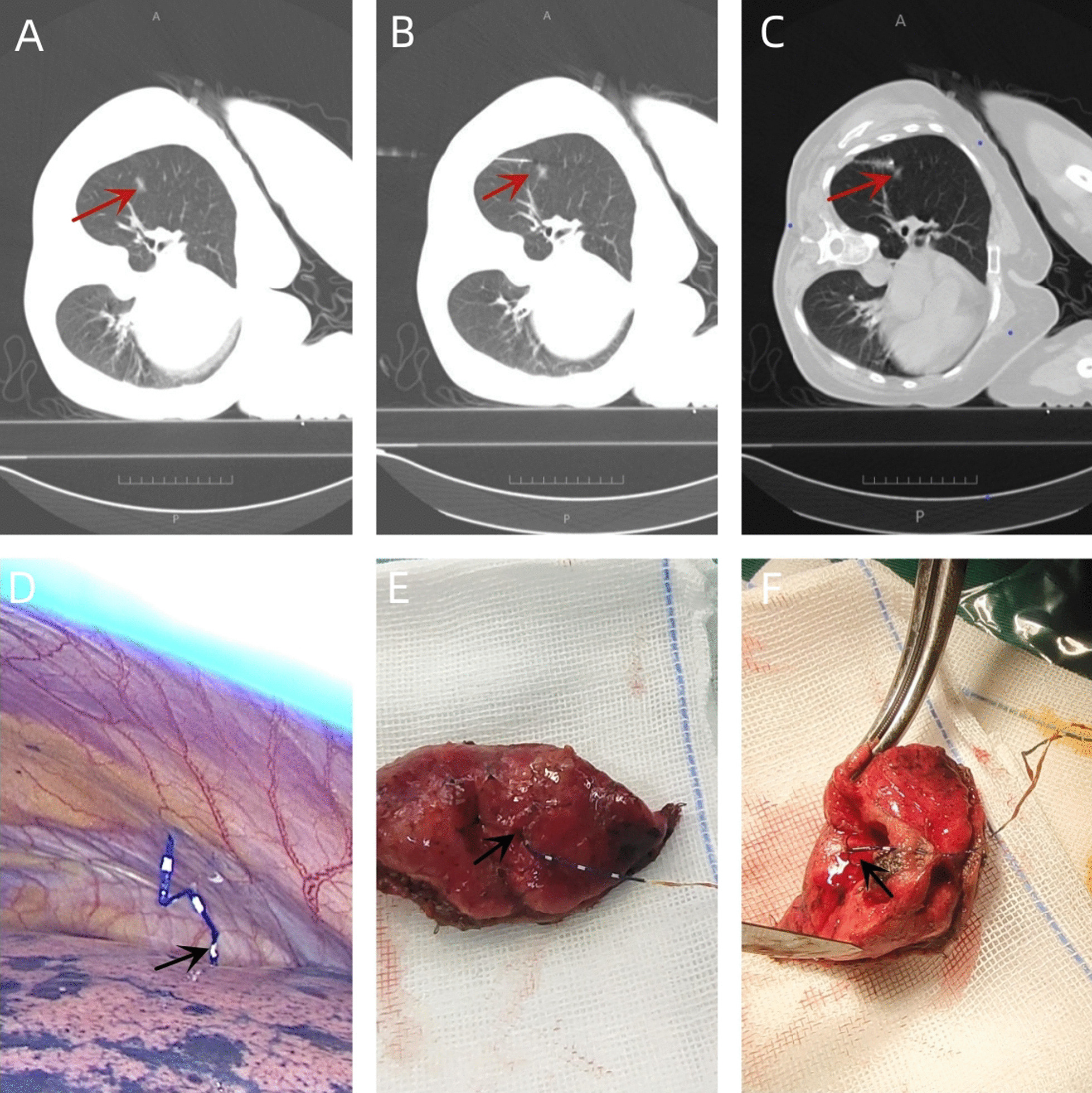
Results: A total of 58 nodules were localized in 50 patients in the localization group, and the localization success rate was 98.3% (57/58). In one case, the positioning pin fell off before wedge resection was performed. The mean nodule diameter was 7.05 mm (range, 2.8-10.0 mm), while the mean depth from the pleura was 22.40 mm (range, 5.47-79.47 mm). There were 8 cases (16%) of asymptomatic pneumothorax, 2 (4%) of intrapulmonary hemorrhage, and 1 (2%) of pleural reaction.The mean operation time of the localization group (103.88 ± 41.74 min) was significantly shorter than that of the control group (133.30 ± 45.42 min) (P < 0.05). The mean intraoperative blood loss of the localization group (44.20 ± 34.17 mL) was significantly lower than that of the control group (112.30 ± 219.90 mL) (P < 0.05). The mean hospital stay of the localization group (7.96 ± 2.34 days) was significantly shorter than that of the control group (9.21 ± 3.25 days).Multivariate binary logistic analysis showed that localization times of small pulmonary nodules in the localization group was an independent risk factor for localization-related pneumothorax.
Conclusions: Our results suggest that the CT-guided hook-wire localization technique is beneficial for localizing small pulmonary nodules. Specifically, it is helpful for the diagnosis and treatment of early lung cancer because it can accurately remove lesions, decrease intraoperative blood loss, shorten operation time and hospitalization stay, and reduce thoracotomy conversion rate. Simultaneous positioning of multiple nodules can easily lead to positioning-related pneumothorax.
Keywords: CT guidance; Hook-wire localization; Pulmonary nodules; Thoracoscopic surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Study on the Application Effect of Three-dimensional Reconstruction Technology in Locating Small Pulmonary Nodules During VATS Surgery.Altern Ther Health Med. 2025 Sep;31(5):180-185. Altern Ther Health Med. 2025. PMID: 38836733
-
Analysis on the application of a CT-guided medical adhesive-based localization method in sublobectomy to ensure surgical margins.BMC Pulm Med. 2025 Jul 2;25(1):305. doi: 10.1186/s12890-025-03762-2. BMC Pulm Med. 2025. PMID: 40604767 Free PMC article.
-
CT-guided hook-wire localization of malignant pulmonary nodules for video assisted thoracoscopic surgery.J Cardiothorac Surg. 2020 Oct 9;15(1):307. doi: 10.1186/s13019-020-01279-9. J Cardiothorac Surg. 2020. PMID: 33036640 Free PMC article.
-
Comparative Effectiveness and Safety of Preoperative Lung Localization for Pulmonary Nodules: A Systematic Review and Meta-analysis.Chest. 2017 Feb;151(2):316-328. doi: 10.1016/j.chest.2016.09.017. Epub 2016 Oct 4. Chest. 2017. PMID: 27717643
-
Evidence for the treatment of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition).Chest. 2007 Sep;132(3 Suppl):94S-107S. doi: 10.1378/chest.07-1352. Chest. 2007. PMID: 17873163
Cited by
-
Preoperative CT-Guided Coil Localization of Lung Nodule Resection: A Single-Center Experience.Cureus. 2023 Jul 26;15(7):e42503. doi: 10.7759/cureus.42503. eCollection 2023 Jul. Cureus. 2023. PMID: 37637515 Free PMC article.
-
[Advancements in Research on Preoperative Localization of Pulmonary Nodules].Zhongguo Fei Ai Za Zhi. 2025 May 20;28(5):385-390. doi: 10.3779/j.issn.1009-3419.2025.101.07. Zhongguo Fei Ai Za Zhi. 2025. PMID: 40506493 Free PMC article. Review. Chinese.
-
Comparison between preoperative hook-wire and liquid material localization for pulmonary nodules: a meta-analysis.Wideochir Inne Tech Maloinwazyjne. 2023 Sep;18(3):401-409. doi: 10.5114/wiitm.2023.130330. Epub 2023 Aug 4. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 37868290 Free PMC article.
References
-
- Lung Cancer Group of the Chinese Medical Association Respiratory, Expert Group of Chinese Alliance Against Lung Cancer. Chinese Expert Consensus on the Diagnosis and Treatment of Pulmonary Nodules (2018 Edition). Chinese Journal of Tuberculosis and Respiratory Diseases. 2018, 41(10):763–771.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
