

Practical considerations for determination of scapular internal rotation and its relevance in reverse total shoulder arthroplasty planning
- PMID: 37020305
- PMCID: PMC10077691
- DOI: 10.1186/s13018-023-03762-0
Practical considerations for determination of scapular internal rotation and its relevance in reverse total shoulder arthroplasty planning
Abstract
Background: Scapulothoracic orientation, especially scapular internal rotation (SIR) may influence range of motion in reverse total shoulder arthroplasty (RTSA) and is subjected to body posture. Clinical measurements of SIR rely on apical bony landmarks, which depend on changes in scapulothoracic orientation, while radiographic measurements are often limited by the restricted field of view (FOV) in CT scans. Therefore, the goal of this study was (1) to determine whether the use of CT scans with a limited FOV to measure SIR is reliable and (2) if a clinical measurement could be a valuable alternative.
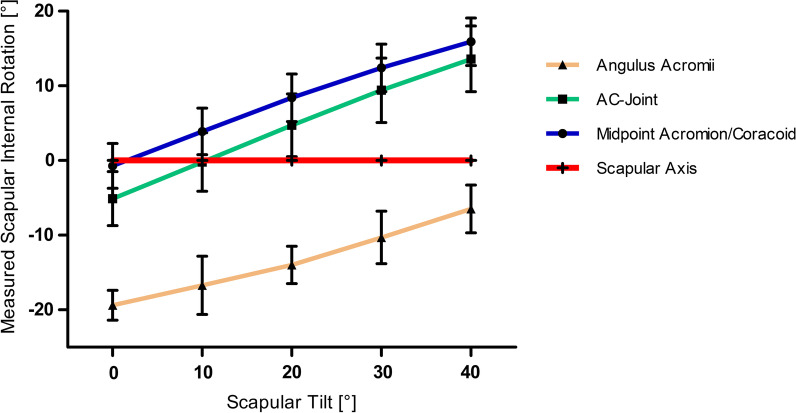
Methods: This anatomical study analyzed the whole-body CT scans of 100 shoulders in 50 patients (32 male and 18 female) with a mean age of 61.2 ± 20.1 years (range 18; 91). (1) CT scans were rendered into 3D models and SIR was determined as previously described. Results were compared to measurements taken in 2D CT scans with a limited FOV. (2) Three apical bony landmarks were defined: (the angulus acromii (AA), the midpoint between the AA and the coracoid process tip (C) and the acromioclavicular (AC) joint. The scapular axis was determined connecting the trigonum scapulae with these landmarks and referenced to the glenoid center. The measurements were repeated with 0°, 10°, 20°, 30° and 40° anterior scapular tilt.
Results: Mean SIR was 44.8° ± 5.9° and 45.6° ± 6.6° in the 3D and 2D model, respectively (p < 0.371). Mean difference between the measurements was 0.8° ± 2.5° with a maximum of 10.5°. Midpoint AA/C showed no significant difference to the scapular axis at 0° (p = 0.203) as did the AC-joint at 10° anterior scapular tilt (p = 0.949). All other points showed a significant difference from the scapular axis at all degrees of tilt.
Conclusion: 2D CT scans are reliable to determine SIR, even if the spine is not depicted. Clinical measurements using apical superficial scapula landmarks are a possible alternative; however, anterior tilt influenced by posture alters measured SIR.
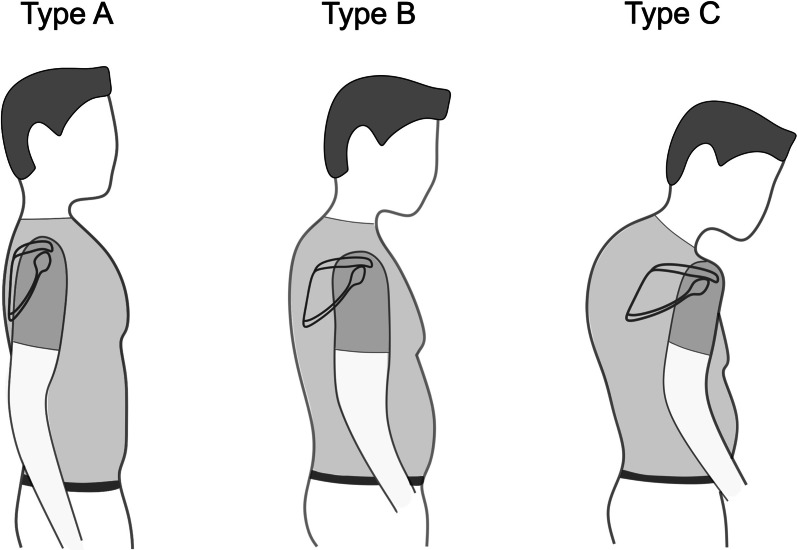
Keywords: Posture types; Reverse total shoulder arthroplasty; Scapular internal rotation; Scapulothoracic orientation.
© 2023. The Author(s).
Conflict of interest statement
PM is a consultant for Arthrex. All other authors declare that they have no competing interests.
Figures






References
-
- Moroder P, Urvoy M, Raiss P, Werthel JD, Akgun D, Chaoui J, et al. Patient posture affects simulated ROM in reverse total shoulder arthroplasty: a modeling study using preoperative planning software. Clin Orthop Relat Res. 2022;480(3):619–631. doi: 10.1097/CORR.0000000000002003. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
