

Multifactorial Analysis of Treatment of Long-Bone Nonunion with Vascularized and Nonvascularized Bone Grafts
- PMID: 37020609
- PMCID: PMC10070005
- DOI: 10.1055/s-0042-1748783
Multifactorial Analysis of Treatment of Long-Bone Nonunion with Vascularized and Nonvascularized Bone Grafts
Abstract
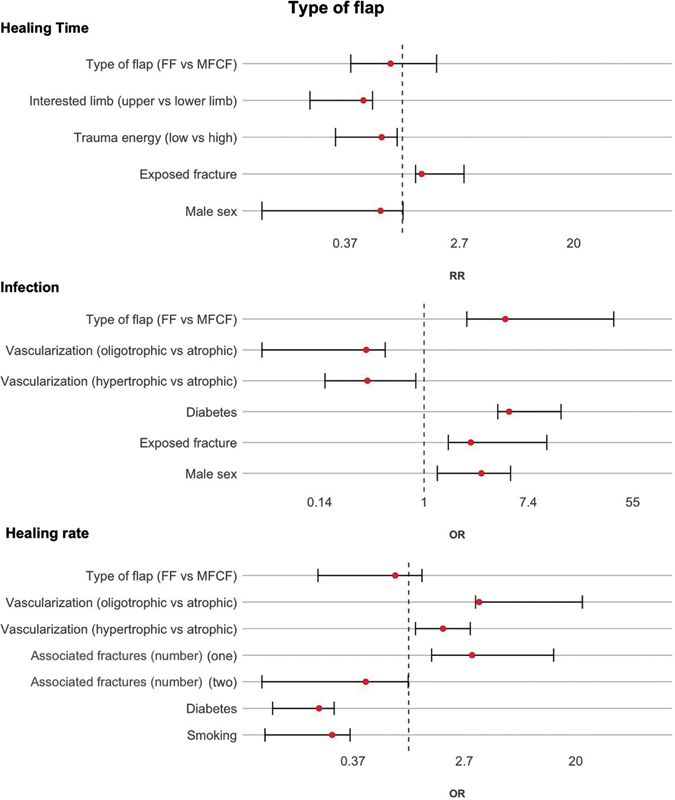
Introduction The purpose of the study was to evaluate the results of treatment of the nonunion of long bones using nonvascularized iliac crest grafts (ICGs) or vascularized bone grafts (VBGs), such as medial femoral condyle corticoperiosteal flaps (MFCFs) and fibula flaps (FFs). Although some studies have examined the results of these techniques, there are no reports that compare these treatments and perform a multifactorial analysis. Methods The study retrospectively examined 28 patients comprising 9 women and 19 men with an average age of 49.8 years (range: 16-72 years) who were treated for nonunion of long bones between April 2007 and November 2018. The patients were divided into two cohorts: group A had 17 patients treated with VBGs (9 patients treated with MFCF and 8 with FF), while group B had 11 patients treated with ICG. The following parameters were analyzed: radiographic patterns of nonunion, trauma energy, fracture exposure, associated fractures, previous surgeries, diabetes, smoking, age, and donor-site morbidity. Results VBGs improved the healing rate (HR) by 9.42 times more than the nonvascularized grafts. Treatment with VBGs showed a 25% decrease in healing time. Diabetes increased the infection rate by 4.25 times. Upper limbs showed 70% lower infection rate. Smoking among VBG patients was associated with a 75% decrease in the HR, and diabetes was associated with an 80% decrease. Conclusion This study reports the highest success rates in VBGs. The MFCFs seem to allow better clinical and radiological outcomes with less donor-site morbidity than FFs.
Keywords: iliac crest bone graft; medial femoral condyle; nonunion of long bone; vascularized bone grafts; vascularized fibular graft.
Society of Indian Hand Surgery & Microsurgeons. All rights reserved.
Conflict of interest statement
Conflict of Interest The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article. Dr. Calcagni reports nonfinancial support from Sobi, nonfinancial support from Medartis, nonfinancial support from Silk Biomaterials, nonfinancial support from DyCare, outside the submitted work.
Figures




Similar articles
-
The medial femoral condyle free corticoperiosteal flap versus traditional bone graft for treatment of nonunions of long bones: a retrospective comparative cohort study.Injury. 2019 Dec;50 Suppl 5:S54-S58. doi: 10.1016/j.injury.2019.10.049. Epub 2019 Oct 21. Injury. 2019. PMID: 31711649
-
Free vascularized fibular bone grafting in the management of femoral neck nonunion in patients younger than fifty years.J Orthop Trauma. 2002 Aug;16(7):464-72. doi: 10.1097/00005131-200208000-00004. J Orthop Trauma. 2002. PMID: 12172276
-
Vascularized bone grafts for the treatment of carpal bone pathology.Hand (N Y). 2013 Mar;8(1):27-40. doi: 10.1007/s11552-012-9479-0. Hand (N Y). 2013. PMID: 24426890 Free PMC article.
-
Vascularized Bone Grafts in Spinal Reconstruction: An Overview of Nomenclature and Indications.Semin Plast Surg. 2021 Feb;35(1):50-53. doi: 10.1055/s-0041-1726101. Epub 2021 May 10. Semin Plast Surg. 2021. PMID: 33994879 Free PMC article. Review.
-
Vascularized bone grafts for upper limb reconstruction: defects at the distal radius, wrist, and hand.J Hand Surg Am. 2010 Oct;35(10):1710-8. doi: 10.1016/j.jhsa.2010.08.006. J Hand Surg Am. 2010. PMID: 20888511 Review.
Cited by
-
The Vascularized Fibula as Salvage Procedure in Extremity Reconstruction: A Retrospective Analysis of Time to Heal and Possible Confounders.Life (Basel). 2024 Feb 28;14(3):318. doi: 10.3390/life14030318. Life (Basel). 2024. PMID: 38541644 Free PMC article.
References
-
- Campbell W C. The autogenous bone graft. J Bone Joint Surg. 1939;21:694.
-
- Ahlmann E, Patzakis M, Roidis N, Shepherd L, Holtom P. Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone Joint Surg Am. 2002;84(05):716–720. - PubMed
-
- Weiland A J, Moore J R, Daniel R K. The efficacy of free tissue transfer in the treatment of osteomyelitis. J Bone Joint Surg Am. 1984;66(02):181–193. - PubMed
-
- Foster R D, Anthony J P, Sharma A, Pogrel M A. Vascularized bone flaps versus nonvascularized bone grafts for mandibular reconstruction: an outcome analysis of primary bony union and endosseous implant success. Head Neck. 1999;21(01):66–71. - PubMed
-
- Soucacos P N, Kokkalis Z T, Piagkou M, Johnson E O. Vascularized bone grafts for the management of skeletal defects in orthopaedic trauma and reconstructive surgery. Injury. 2013;44 01:S70–S75. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous