

Recurrent renal secondary hyperparathyroidism caused by supernumerary mediastinal parathyroid gland and parathyromatosis: A case report
- PMID: 37021088
- PMCID: PMC10067725
- DOI: 10.3389/fsurg.2023.1135596
Recurrent renal secondary hyperparathyroidism caused by supernumerary mediastinal parathyroid gland and parathyromatosis: A case report
Abstract
Background: Surgical parathyroidectomy (PTX) is necessary for patients with severe and progressive secondary hyperparathyroidism (SHPT) refractory to medical treatment. Recurrence of SHPT after PTX is a serious clinical problem. Both supernumerary mediastinal parathyroid gland and parathyromatosis are the rare causes of recurrent renal SHPT. We report a rare case of recurrent renal SHPT due to supernumerary mediastinal parathyroid gland and parathyromatosis.
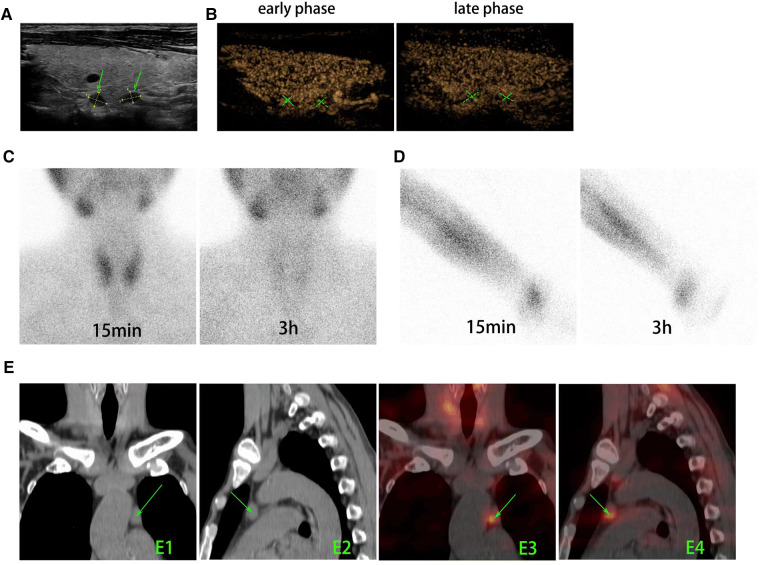
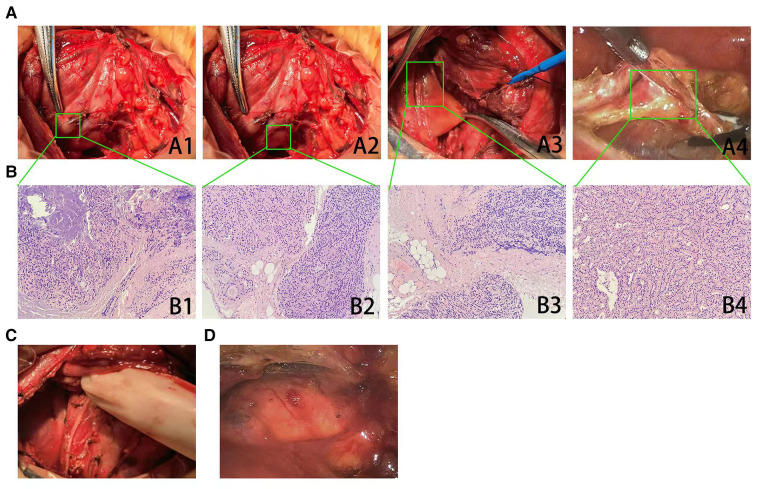
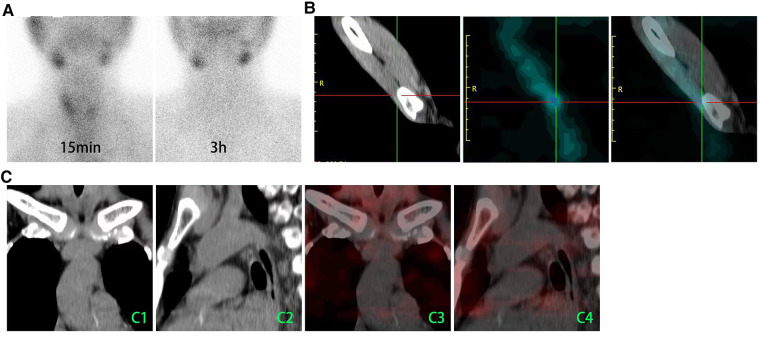
Case presentation: A 53-year-old man underwent total parathyroidectomy with autotransplantation due to the drug-refractory SHPT 17 years ago. In the last 11 months, the patient experienced symptoms including bone pain and skin itch, and the serum intact parathyroid hormone (iPTH) level elevated to 1,587 pg/ml. Ultrasound detected two hypoechoic lesions located at the dorsal area of right lobe of the thyroid gland, and both lesions presented as characteristics of hyperparathyroidism in contrast-enhanced ultrasound. 99mTc-MIBI/SPECT detected a nodule in the mediastinum. A reoperation involved a cervicotomy for excising parathyromatosis lesions and the surrounding tissue and a thoracoscopic surgery for resecting a mediastinal parathyroid gland. According to a histological examination, two lesions behind the right thyroid lobe and one lesion in the central region had been defined as parathyromatosis. A nodule in the mediastinum was consistent with hyperplastic parathyroid. The patient remained well for 10 months with alleviated symptoms and stabilized iPTH levels in the range of 123-201 pg/ml.
Conclusion: Although rare, recurrent SHPT may be caused by a coexistence of both supernumerary parathyroid glands and parathyromatosis, which should receive more attention. The combination of imaging modalities is important for reoperative locations of parathyroid lesions. To successfully treat parathyromatosis, all the lesions and the surrounding tissue must be excised. Thoracoscopic surgery is a reliable and safe approach for the resection of ectopic mediastinal parathyroid glands.
Keywords: case reports; hyperparathyroidism; parathyromatosis; recurrence; secondary; supernumerary parathyroid glands.
© 2023 Li, He, Cheng, Cao, Wang, Tang and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Persistent secondary hyperparathyroidism caused by parathyromatosis and supernumerary parathyroid glands in a patient on haemodialysis.BMC Nephrol. 2020 Jul 6;21(1):257. doi: 10.1186/s12882-020-01917-3. BMC Nephrol. 2020. PMID: 32631272 Free PMC article.
-
Unusual recurrent renal secondary hyperparathyroidism caused by hyperplastic autograft with supernumerary parathyroid adenoma: A case report.Medicine (Baltimore). 2019 Jun;98(24):e16077. doi: 10.1097/MD.0000000000016077. Medicine (Baltimore). 2019. PMID: 31192970 Free PMC article.
-
Parathyromatosis as a cause of recurrence primary hyperparathyroidism: A case report.Int J Surg Case Rep. 2021 Mar;80:105689. doi: 10.1016/j.ijscr.2021.105689. Epub 2021 Feb 22. Int J Surg Case Rep. 2021. PMID: 33752295 Free PMC article.
-
Parathyromatosis: a cause for recurrent hyperparathyroidism.Endocr Pract. 2001 May-Jun;7(3):189-92. doi: 10.4158/EP.7.3.189. Endocr Pract. 2001. PMID: 11421566 Review.
-
Parathyromatosis: a very rare cause of recurrent primary hyperparathyroidism - case report and review of the literature.Ann R Coll Surg Engl. 2019 Nov;101(8):e178-e183. doi: 10.1308/rcsann.2019.0105. Epub 2019 Sep 11. Ann R Coll Surg Engl. 2019. PMID: 31509000 Free PMC article. Review.
Cited by
-
Advantages of total parathyroidectomy in patients with secondary hyperparathyroidism induced by end stage renal disease.Front Endocrinol (Lausanne). 2023 Nov 22;14:1191914. doi: 10.3389/fendo.2023.1191914. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38075043 Free PMC article.
-
Recurrence hyperparathyroidism caused by synchronous parathyroid carcinoma and parathyromatosis in a patient with long-term hemodialysis.BMC Nephrol. 2023 Oct 4;24(1):293. doi: 10.1186/s12882-023-03328-6. BMC Nephrol. 2023. PMID: 37794407 Free PMC article.
-
Recurrent secondary hyperparathyroidism due to a gradually increasing intrathyroidal parathyroid adenoma in a fifth parathyroid gland of a patient undergoing long-term haemodialysis: Road to evil.BMC Nephrol. 2025 Feb 3;26(1):53. doi: 10.1186/s12882-024-03878-3. BMC Nephrol. 2025. PMID: 39901080 Free PMC article.
-
Parathyroid Carcinoma Complicated by Parathyromatosis and Refractory Hypercalcemia.Cureus. 2024 Oct 28;16(10):e72584. doi: 10.7759/cureus.72584. eCollection 2024 Oct. Cureus. 2024. PMID: 39478762 Free PMC article.
References
-
- Bozic M, Diaz-Tocados JM, Bermudez-Lopez M, Forné C, Martinez C, Fernandez E, et al. Independent effects of secondary hyperparathyroidism and hyperphosphataemia on chronic kidney disease progression and cardiovascular events: an analysis from the NEFRONA cohort. Nephrol Dial Transplant. (2022) 37(4):663–72. 10.1093/ndt/gfab184 - DOI - PubMed
-
- Ogata H, Kumasawa J, Fukuma S, Mizobuchi M, Kinugasa E, Fukagawa M, et al. The cardiothoracic ratio and all-cause and cardiovascular disease mortality in patients undergoing maintenance hemodialysis: results of the MBD-5D study. Clin Exp Nephrol. (2017) 21(5):797–806. 10.1007/s10157-017-1380-2 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials